CONTENTS
CHAPTER
FIVE � GENERATING FERTILE SOIL AT FRASER HOUSE
PRIMARY-GROUP
THERAPY - �FAMILY-FRIENDS THERAPY� - �HOUSEHOLD THERAPY�
Utilizing
Collective Social Forces
ON NEVILLE�S
ROLE AS LEADER AND HIS GROUP PROCESSES..
On the Side of
Constructive Striving
The Flexible
Enabler - Control and Abandon � Surrender and Catch
Differing
Patterns of Interaction
Cliques,
Factions and Use of Space
Functionally
Mingling Dysfunction
SOCIAL
CATEGORY BASED SMALL GROUP THERAPY
What Do You
Think About Trade With Asia?
PSYCHIATRIC
RESEARCH STUDY GROUP
A FOLLOW-UP SERVICE
AND LIAISON WITH OUTSIDE ORGANIZATIONS.
MARGARET MEAD
VISITS FRASER HOUSE
CASE HISTORIES
SHOWING GLIMPSES OF THE FRASER HOUSE MODEL IN ACTION
The North
Shore Bus Depot Gang
REFLECTING ON
FRASER HOUSE �TREATMENT� APPROACHES
DIAGRAMS
Diagram 1 Layout of Big Group showing two tiered platforms.
Diagram 2 The Cleavered Unity of Big Group Was Then Cleavered Into Ten
Small Groups
Diagram 3 The Circular Concept
Diagram 5 The use of space in Big Group
DRAWINGS
Drawing 1 A Sketch of a Fraser House Small Group
FIGURES
Figure 1 Constructive Emotional and Constructive Administrative Support
Figure 2 Examples of Research Questions Asked in Fraser house
PHOTOS
Photo 1 The room at Fraser House Where Big Group Was Held
Photo 3 The Sheer Cliffs at the Gap
Photo 5 Patients building the Fraser House bowling
green in the Sixties.
Photo 6 Photo taken in 2000 showing brick retaining wall
Photo 7 These Are the Grounds Outside Fraser House Where the Horse Grazed
Photo 8 The Rear of the Building Where the Gang Hid Their Gear.
ORIENTATING
This Chapter outlines Family-Friends Therapy and Big Group Therapy process along with some of Neville�s leader
roles and processes during Big Group and Small Groups. A number of other
innovative change processes are specified including Small Group Therapy with
membership based on a set of rotating sociological categories. Two case studies
provide a feel for Fraser House in action. The Chapter concludes with a
discussion of Neville�s adaptation of his father�s Keyline to Cultural Keyline
PRIMARY-GROUP
THERAPY - �FAMILY-FRIENDS THERAPY� - �HOUSEHOLD THERAPY�
Typically, patients
arrived at Fraser House with a small (2-7 people) dysfunctional
family/friendship/workmate network. Neville said that the assumption and the
experience of Fraser House people was that the individual patient was
fundamentally a part of this dysfunctional social context. Patient pathology
was inter-related, inter-connected and inter-woven with the pathology of the
social (family/friendship) network in which the patient was enmeshed. The Unit�s
�treatment� aim was to increase the patients� role-taking functionality and
psychological comfort towards their returning to functional life in their local
community with an extended and functional
family/friendship/workmate network,
typically of around seventy
people! Processes whereby most patients achieved this are discussed later
in this Chapter.
According
to Chilmaid in August 1999, there was not so much a �treatment program�, more
that everyone new who had what problems. Treatment tended to be context driven
and informal rather than formal and planned. Notwithstanding this frame, both
the Admissions Committee and the Progress Committee did identify the �big�
and� �small� chunks that needed resolving
and these were made known to the community-as-therapist.
��
In his paper, �Sociotherapeutic
Attitudes to Institutions�, and consistent with creating �cultural locality�,
Neville wrote that mental health professionals ��must aim at allowing the
outside culture into the institution (Yeomans 1965 Vol. 12, p. 46, 60-61)�. One of
the change processes at Fraser House was called Primary-Group Therapy. It was
also called �Family-Friends-Workmate Therapy� and �Household Therapy�. This
therapy involved attendance of a patient�s family, friends and workmates as outpatients
at Big Group and Small Group therapy. One of Neville�s monograph�s
reports that, �relatives routinely attended groups in 1961; it also mentioned
that relatives friends and workmates attended the Unit (Yeomans 1965, Vol. 4. p. 2-4).
There was a rule implemented that
patients and their families and friends were required to attend twelve
groups before the patient�s admission. This rule ensured prospective
patients knew that families and friends regular attendance was a requirement
Additionally, this rule had the effect of having people absorbed into the
community before becoming residents or outpatient friends and relatives
of residents with all the advantages flowing from this close fit.
This is discussed in the
next two sections. Given that the patient and his family-friend-workmate
network was the focus of change, Primary-Group Therapy was fundamental and a requirement
for a patient being accepted into Fraser House.
During Big Group everyone was �in therapy�.� Visiting Family, workmates and friends would
�sign on� as outpatients. In an April 1999 conversation with Bruen he said that
while it was not �spelt out� to staff that they too were �in therapy�, a person
could not be in Big Group and not be
�in therapy�; it was just so �dense� that people had to have psychosocial and
emotional shifts occur. This view was confirmed by Neville, Cockett and
Chilmaid. This is resonant with Maxwell Jones comment that anyone in Fraser
House had to change (Clark and Yeomans 1969,
Preface).
Family, friends and
workmates attending small groups would be regularly split into differing groups
by design, and because of the dividing of groups by sociological category.
Pathological families who were patients at Fraser House were regularly split up
(the cleavering of pathological unities) during day-to-day life in the Unit.
For example, they would not be allowed to sit next to each other at mealtimes.
They would attend differing small groups. This cleavering was to allow space
for new behaviors and the taking on of new roles towards building a more
functional unity. This carefully planned cleavering and strategic linking of
the parts was a feature of a process Neville called mediation therapy where
mediation is an adjective hinting at the process involved in re-constituting
functional relating in dysfunctional family-friendship networks.
There was also the age
based inter-generational cleavering, the married/single cleavering and the
mad/bad cleavering (under-controlled/over-controlled and the
under-active/over-active). There was the cleavering of the mad/bad between all
the diagnostic categories represented. Recall that in Firth�s terms cleavered
unity was a feature of Tikopia�s life. A list of the diagnostic categories
represented in Fraser House at one point in time is shown in Appendix 3. The
cleavered unity of Big Group was continually cleavered into differing small
groups that rotated each weekday through the various sociological categories.
As required, special groups were convened outside of structured group time to
work through crises, or for special purposes. These were at times run by the
patients without staff attending. Typically there were around twelve special
groups a week.
FAMILY
THERAPY
Family
units were set up early in Fraser House�s history. Fraser House was the first
unit in Australia to be use family therapy, family-friends therapy and full
family residential therapeutic community. Recall that there were eight family
units that included cots for young children. Virginia Satir was around the same
time pioneering family therapy in the United States (Satir
1964; Satir 1972; Satir 1983; Satir 1988). The Fraser House
experience was that among patient�s networks, inter-generational dysfunction
was common and that people within �pathological families� were often being
rewarded for deviance.
Independent
of genetic psychosocial pathology (inheritance), aspects of the patterns of
daily interaction (heritage) were helping to constitute and sustain pathology,
often among three generations. There was also evidence that in many families,
the heritage of pathology went further back than the three generations. This
evidence was consistent with Neville�s requirement of have a patient�s
multiple-generation family-friendship network attend the Unit as outpatients.
BIG GROUP, THE BIG MEETING,
COMMUNITY MEETING, LARGE GROUP PSYCHOSOCIAL THERAPY, COLLECTIVE THERAPY, BIG
GROUP THERAPY
Utilizing
Collective Social Forces
All the above terms were
used to refer to the whole community meeting held twice a day during weekdays.
Morning Big Group was held from 9:30 AM to 10:30 AM.� Evening Big Group was from 6:30 PM till 7:30
PM. These were followed by a 30-minute tea break. Then everyone reconvened
separated into Small Groups.
In Neville�s paper, �Collective Therapy �
Audience and Crowd� (Yeomans 1966), Neville wrote, �the skilled use of
collective forces is one of the paramount functions of the socio-therapist and
such skills are defined by the team as, �Collective Therapy�. In his paper,
�Sociotherapeutic Attitudes to Institutions� Neville wrote, �Collective therapy,
both audience and crowd, utilizes social forces in the patients� primary group (Yeomans 1965 Vol.
12, p. 46, 60-61).� Neville engaged
all involved in Fraser House in recognizing, understanding and utilizing these
social forces. The Fraser House Handbook written by patients (excerpts in
Appendix 05) also refers to audience and crowd behavior, especially contagion,
being a central aspect of Big Group (Yeomans 1965 Vol. 4,
p. 18-20, 50-54)
Twice a day during weekdays all people
in Fraser House gathering in what was called Big Group. For a time it involved
around 100 people (reference) and then it grew to around 180 people. It peaked
at 300 on one occasion.� All these people
would be crammed into a rather small room - a mixture of the very mad and the
very bad patients, along with their (often strange) friends, workmates and
relatives as outpatients, together with all
the staff on duty at the time, as well as guests. Often there were visitors to
Big Group in addition to friends and relatives of patients. These included
people who attended the Psychiatric Research Study Group, people Neville had
invited from the media, people Neville connected with through his extensive
outreach talk schedule, students and others who made requests to attend.
Members of Alfred Clark�s External Study team would also attend. On one
occasion a TV crew from the ABC came and filmed a section of Big Group. I was
not able to track down this film in the ABC archives. Some of the many
organizations that had their people attend Big Group to learn group skills are
mentioned later.
Some patients had jobs that they would go to during the day. They
would attend evening Big Group. Once Big Group started, the ground rule was
that no one left before it was
finished. A toilet was available within the room behind a screen. Two staff
were assigned to be recorders, one for content, one for process. Big Group process
records were kept in a very large hard covered red book. This assignment was
rotated to improve staff�s attending and process observing skills. This record
was referred to during staff discussion in the tea break following Big Group. I
have been unable to trace this red book. It seems that no records exist of any
aspect of Fraser House in Government records. Neville and Margaret Cockett both
confirmed that there were powerful forces very determined to see all trace of
Fraser House eliminated.

Photo 1 The room at Fraser House Where Big Group Was Held
The
Fraser House Handbook written by patients (Yeomans 1965, Vol. 4, p. 1-54) confirms that during the staff discussion in the tea break following Big Group
the two official observers for the meeting used the Red Book to give their
report to staff followed by comments by all staff members present, including
the Group Leader/Therapist.
�The
points assessed were: mood, theme, value and interaction, therapists role and
techniques employed. From these �post-mortems� comes much of the knowledge
needed.�
�The
aim must be always to look at the community in the �BIG� � as a whole and this
certainly is no easy matter (Yeomans
1965, Vol. 4, p. 51).�
Neville always led Big Group when Fraser House was first set up.
After a time, others began to get a feel for how to do it. Big Group was then
also taken by medical staff. Later on, some nurse leaders also lead Big Group.
As mentioned, three of the people I interviewed for this research, Cockett,
Bruen, and Chilmaid all ran Big Group many times. After Neville left Fraser
House in 1968 some Big Groups were even run by skilled patients. This was
reported by Warwick Bruen in a conversation in April 1999. According to Neville
and Margaret Cockett, Margaret Mead ran Big Group very skillfully when she
visited Fraser House. Mental health was one of Mead�s passionate interests as
an early head of the World Mental Health Federation (2002).
Evening
groups catered for friends and relatives who found it difficult to come during
the day, and for inpatients that worked during the day. The evening Big Groups
and follow-on small groups were voluntary, though well attended (query this �
was it voluntary for outpatients, or all). Thursday morning Big Group was
�administrative only�.
During an
interview/conversation with Neville in April 1999 he stated that any attempt to
bring up an administrative matter in a therapy group was deemed to be �flight�
and was interrupted with compassionate ruthlessness. Any attempt to bring up a
therapy matter during an administrative group was deemed to be �obstruction�
and deferred.
Preventing
Session Creep
All therapy sessions at Fraser House were set strictly at a length
of one hour. Timing of the following tea break and the one-hour small group was
strictly adhered to. When the hour was up they stopped, even if it was in mid
sentence. This was specified by Neville after reading articles that therapy
sessions get progressively longer once over forty-five minutes. This material
comes from a discussion with Neville on 30 June 1999. What tends to happen is
that people tend to leave opening up to the last five minutes, and when they do
open up there is some pressure there to work through something and the session
is extended. Next time nothing much happens till the last five minutes of the
longer period, and so the session extends even further.
To stop this �session creep�, Neville set sixty minutes as the
non-negotiable length. This worked. Typically, people did have things that they
wanted to vent during Big Group. After this �set time length� protocol was
established, people with issues would be clamoring to have them heard at the
very start of Big Group. People knew that if people procrastinated and then it
started hotting up at the 55-minute mark, it would then stop a few minutes
later. Everyone soon learned to do things faster. In a very short time Big
Group would get underway immediately.�
Soon it started itself. There were always one or two people trying to start
before people arrived. �Solve my problem.� �He is harming me!� �Criminals�
would want to attack. An anxious person would want support. A �criminal� would
say he is being blamed wrongly.�
Administrative
Big Group
During the Thursday
morning Big Group meeting, ward administrative matters were discussed and
patient committee elections were held under the auspices of the Parliamentary
Committee. Reports were also received from the other patient committees.
Completely
superficial matters and domestic problems could be brought up during the final
stages of the Thursday morning administrative Big Group meeting. All Big Group
meetings except on Thursday morning were designated �therapy only�. Problems of
ward routines were prohibited except when they involved very intense emotional
relationships reflecting treatment related difficulties.
Big
Group Layout
So that everyone
could see everyone at Big Group, moveable wooden tiers were set up along each
of the long sides of the Big Group room. The room was laid out as depicted in
Diagram 06.� Staff, Patients and
Outpatients were all mixed together. A raised podium was set up at the far end
for the two recorders who kept a transcript of the proceedings.
It
is interesting to gaze for a time at the depiction below of all the people in Big
Group. One may get a sense of the dynamic of the number of people in the room
and the cleavage between staff, patient and visitors. The Big Group room was
rather small for the numbers that crammed into it - around 8 meters by 16
meters. Typically, the attendees sat in two rows along both of the long sides. An opening was left near the doors where seats were
reserved for latecomers. Attendees were all jammed in shoulder to shoulder. The
peak attendance was around three hundred and the room must have been
crammed as it is a relatively small room. Mostly it
was around 100-180. . When the numbers exceeded 180, there would be
three rows along one or both of these long sides. These
attendance figures were mentioned by Phil Chilmaid in an April 1999 interview.
The Sixties were a time
when women were generally quiet in men�s presence and would be quiet if men
were talking. In other hospital environments this reticence to talk in the
presence of men tended to apply to both female staff and female patients. An observation
made by Phil Chilmaid during an August 1999 discussion was that at Fraser
House, females were often passionate in groups and would often catch the
group�s focus and hold the floor.
Outside of Big Group, all involved in Fraser House were dispersed
throughout the quarter of a kilometer long complex. In squeezing the total
community and visitors into Big Group Neville was creating concentrated
cultural locality. Everyone was part of the shoulder-to-shoulder crowd;
everyone was audience and spectator. And everyone knew they would become the
center of the crowd�s focus and that this could happen at any time.
Being the focus of Big Group was a very potent extraordinary socio-emotional
experience. Neville was very adept at creating the unexpected sudden shift in
group focus. That anyone could become the focus of group attention at any
moment served to create and maintain tension in the group.
In
Diagram 05 male/female, staff/non-staff and inpatient/outpatient cleaverages
are shown by code.
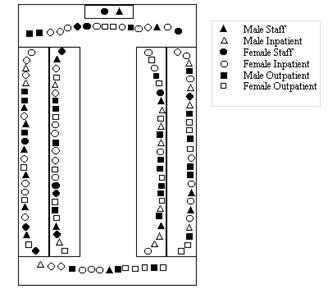
Diagram 1 Layout of Big Group showing two tiered platforms.
Neville is depicted as the black triangle in the
middle of the lower row.

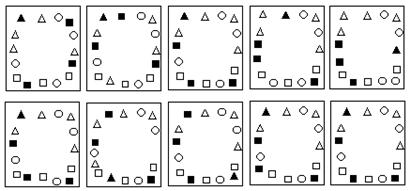
Diagram 2 The Cleavered Unity of Big Group Was Then Cleavered
Into Ten Small Groups
Diagram 3 The Circular Concept
A
Mood That Attunes
A key part of the Big Group reality
was maintaining a �healing environment� that was a �natural growth force�. The
German word �stimmung� is apropos. Stimmung (Pelz 1974, p.89-90) has as one of its meanings, � a mood
that attunes people together�. Within Big Group, Neville set up processes
whereby the collective stimmung that was maintained for the time together was
tuned to healing (Pelz 1974, p. 89-90). However this did not necessarily
mean gentle caring and kindness. Healing often entailed what Neville called,
�ruthless compassion�.� Healing was at
times rugged and relentless. It was at times exhilarating and at other times it
was emotionally draining. In separate April 99
discussions with Neville, Warwick Bruen and Phil Chilmaid, they all confirmed
that Big Group was very tightly structured and that no one liked it - staff and
clients alike. At the same time it was widely acknowledged among both patients
and staff that Big Group was very important - a crucial aspect of the Fraser
House change-work.
The Big Group was not unstructured
like T Groups of the late sixties (Dean 1971); rather, it was very tightly
structured by Neville and the others who followed Neville�s modeling. Big Group
was run like a meeting (Yeomans 1965, Vol. 4, p. 18, 50-54). The patients wrote a detailed
handbook on the role of the Fraser House Nurses and the Conduct of Groups in
Fraser House. It is an extraordinary document, given that it was the patients
who wrote it. However, when it is considered that the patients were the primary
source of training of trainee psychiatrist in community psychiatry, that they
specified the nurses� role and group processes in the Handbook all fits and is
fitting. In writing about group process the handbook states:
��The first essential in taking a group is to
see it as a meeting and like all meetings, there is a need for a chairman to
conduct affairs and keep issues to the point. �The function of the therapist is
to see that the group functions as a group. Be directive. The group could
function well if the chairman adopts a completely passive and wordless role (Yeomans 1965, Vol. 4, 17-20,� 50-54)
The
Patient�s papers on the Nurses Role and Big Group Process are in Appendices 4
& 5.
Any destructive
non-ecological behavior was interrupted. One criticism of T Groups was that
destructive non-ecological feedback was often happening with destructive
consequences. Within Fraser House non-ecological behavior was regularly
occurring because of the nature of the patient/outpatient population. However
this behavior was continually interrupted with ruthless compassion. Examples of
the use of �pattern interrupt� are included later (Hanlon
1987).
Big Group was edge stuff, hence liminal - threshold stuff towards new
constructed realities and contexts. The concept �liminal� is from limin meaning
the threshold or doorstep. It is embedded in the word �preliminary�. This concept is discussed in Chapter Nine. Bruen
commented in April 1999 that Big Group was �exhausting for all present� and
that the leader had to be �really on the ball� and �aware of everything�.
The Fraser House Handbook
written by patients includes to following comment on Big Group process:
�When both the staff and
patients are working well together in the Unit, a peak of enthusiasm is reached
at times when everyone sees almost any move at all as being gainful. New
enterprises are embarked upon with an eagerness that is almost inspired and
success is a certainty.
Again, when as a whole the
big group is swayed by frustration, - contagious aggression and excitement
result; just as contagious as the feelings of fear and panic experienced due to
shared threat anywhere (Yeomans 1965, Vol. 4, p. 51)�
The patients writing the handbook note
that theories of behavior of crowds and audiences apply to Big Group. Further discussion on tuning is contained in
Chapter Six. Creating a collective mood tuned to healing that colors the
collective reality as healing, is itself therapeutic. Within Fraser House, the
realized (in the two-fold sense of �made real� and �understood�) reality/context,
the shared meanings about �what we are here for�, and the collective mood, were
all healing. All participants (apart from newcomers) shared memories of
previous Big Groups where healing had occurred in the shared cultural locality
of the Unit�s Big Group Room. The very space in the room had become healing
space. Healing memories were anchored to this space (Dilts, Grinder et al. 1980, p.
119-151; Lankton 1980, p. 56-60, 70-72, 74, 90-104, 109, 113-116, 118; Bandler,
Grinder et al. 1982, p. 53, 107, 109-110, 150, 165, 175-176, 180-185, 187-188,
193, 198; Hanlon 1987). �Here we are altogether again for
more of this, �whatever it is�!� It was into this shared mood/reality - this
very special stimmung space - that the mad and bad were entering - not just any
old space. This is resonant with Indigenous notions of Special Places and
Sacred Places. It is also resonant with Aboriginal Geoff Guest�s storytelling
place discussed in Chapter Nine (Petford Working Group 2000).
Neville�s perspective
(isomorphic with Milton Erikson�s (Hanlon 1987)) was that people can only do their best, and for mad and bad
people, their best is typically pathological. Often a pathological part of
their repertoire is the only defense they have in particular contexts. To take
that part away from them would leave them defenseless. Functional and hence
more adaptive parts can be added to
repertoires so problematic resources can be used rarely and ecologically. For
example, given a wider range of relating skills, the child�s �withering
comment� that shatters her playmates� can be reserved for the adult �sleaze�.
Given the prevalence of
pathology, Big Group as �healing stimmung� was still riddled with people doing
their best with pathological repertoires, including dysfunctional beliefs about
the world and each other, as well as problematic values, attitudes and habits
and pervasive self-doubt. All of these were being constantly held up to
community scrutiny and challenged. Neville had highly refined competences to
ensure ecology in this dysfunctional seething. This is discussed later in this
Chapter.
A lot of Big Group was like theatre
with vocal people sometimes being rather passionate and rowdy. This was
attested to by Neville and Bruen in April 99. Big Group meetings were sometimes
extremely frightening and challenging. Despite this, as said before, the
context was framed as healing and very tightly controlled.�
ON
NEVILLE�S ROLE AS LEADER AND HIS GROUP PROCESSES
On
the Side of Constructive Striving
As an aid to getting a feel for how Big Group worked and fitted in
with other aspects of the Fraser House milieu I will divert from discussing Big
Group to outline firstly some of Neville�s roles as leader and secondly his Big
Group processes.
Neville�s process for
working with destructive non-ecological behavior was as follows. He was
continually scanning everyone and various factions to sense where everyone was
at (Bruen in April 1999). Whenever Neville was with more than one person, he is
always on the side of the �constructive striving� of everyone present - their
ecological bits. Examples are included later. This process may be termed
�ecology therapy�.� The essence of this
therapy is that Neville never took sides verbally or non-verbally (Yeomans 1965, Vol. 5, p.
66). This is isomorphic with
the Keyline principle, �make use of the free energy in the system�. When
carrying out therapy with family and friends within Big Group, Neville did not
take the side of any one person. Rather, he took the side of, or supported the healthy component of a role in the
relationship between the individuals concerned in that unfolding context.
Neville discussed his process in a monograph entitled, �The problem of Taking
Sides� (Yeomans 1965, Vol 5, p. 46-47).
When working within the intra-psychic
structure of any one person in the family group, Neville supported certain role
behaviors of the particular individual and not other role behaviors. More
specifically, he supported the normal component of certain roles undertaken by
the person in the particular context. Neville did not take sides between the
two or more individuals, even though typically they may be attempting to make
him do this.
Neville was constantly supporting the positive component in role
relationships, and in any one individual in the role relationship - that
person�s positive role behavior component. Using this process, it was
surprising easy for Neville to flow very comfortably through the most
potentially disturbing of family quarrels and conflicts. Neville was supporting
the normal component of their role relationships, and consequently the normal
component of the intra-psychic role structures, Neville was, intra-psychically
speaking, supporting the normal sub-total of roles in the individual and the
group. At the same time, Neville was not supporting and condoning the abnormal
role part functions of any in the group.
Looked at from the perspective of a
person�s total personality, Neville was personally supporting each member of
the group as a person, while fundamentally not supporting nor condoning
anyone�s abnormal behavior. Each member of the group was accepted. Everyone�s
abnormal behavior was rejected. The tension in each individual within the
family/friendship sub-group was thus supported towards the normal. For example,
let�s say that in a couple, the woman was the more dominant partner. During any
discussion or argument between the two, any masculine (Yang) strivings in the
man would be supported by Neville while �female�
(Yin) strivings in the male were actively rejected, by implication rejected, or
at least not supported. Any feminine
(Yin) striving in the wife would have being supported. In another context and
with the same couple, Neville may support the feminine (Yin) aspect of the male and the male (Yang) aspect in the
female because in current unfolding context that emphasis would support towards
the normal.
What Neville was actually
doing was changing his position as a function of the particular roles that were
being attempted by one of the partners in the argument. Neville was always
supporting the context specific healthy role functions.� A colleague David Cruise pointed out the resonance of the words of the Henry
Mercer song (Mercer 2000):
Accentuate
the positive
Eliminate
the negative
Latch
on to the affirmative
Don't
mess with Mister In-Between
In this context, Neville was a positive,
�Mr. In-between and according to all of my interviewees, he was so far ahead of
everyone else in his strategic ruthless compassionate caring that it was best
not to �mess� with him if you were into tearing down wellbeing.
Typically, people�s faith and trust in
Neville continued in spite of his apparent siding with one or the other. They
stayed in the group therapy and come back for more. Also, people tended to have
no idea that Neville was using this process of supporting each person as
�person�, supporting their �ecological bits� and not supporting or rejecting
the non-ecological bits. While at times being compassionately ruthlessness,
Neville would often use subtlety and deftness - drawing on his Aboriginal
Yolgnu experience of behaviors mirroring the ebb and flow of the tide. At
appropriate times Neville would gently move on something. At other times
Neville would gently withdraw. At other times he could be compassionately
ruthless. Neville let the context be his guide. In all this, he excelled at
maintaining rapport with others. This does not mean
that others necessarily agreed with, liked, accepted, or understood Neville �
rather, I use �rapport� to connote that there remained a melding energy between
Neville and others even in the presence of disagreement, dislike,
non-acceptance and non-understanding. Often Neville would intentionally get
people so that they detested him and were furious with him and still they would
continue engagement.
In Big
Group, if anyone was bitching about another person present, Neville engaged and
then immediately interrupted the attacker and suddenly withdrew rapport and
switched full attention to the person being attacked, and ignored the attacker,
and possible the ongoing attacking. This sudden withdrawal of rapport from the
attacker was all the more potent because Neville�s prior report was so strong.
At the same time he would continue to monitor the attacker as part of continual
meta-scanning of the whole group and group process. He may provide support and
comfort, and respond to any constructive striving of the victim. This behavior
�rewarded� the victim and was �punishing� the attacker. Sometimes he may
isolate out and focus on the constructive and ecological bit(s) of the
attacker�s behavior and use this to interrupt the destructive aspects. Neville
was very adept at this rapid pattern interrupt to non-ecological behavior.
Aspects of the interrupt process may include the sudden removal of gaze, the
rapid turning of eyes, head and body away from the attacker, the cessation of
Neville�s attention (as perceived by the attacker), perhaps the hand up, �stop
now� hand gesture of the traffic policeman, the non-acknowledgment of the
attacker�s words and being-in-the-room, and the engagement of the �victim� as
Neville�s (and the Groups) new center of attention. Typically, the victim
became the new center of the group-as-audience�s attention and the attacker was
for the time, �excluded� by the Group process. This was an example of Neville�s
use of social forces. This sudden withdrawal of being the center of the Group�s
attention, the supports to the attacker�s �taken-for-granted what�s happening�-
this �denial of the attacker�s reality� - typically creates an internal
�interrupt� to their state and functioning. Often they go into momentary
confusion. Often
the �state� of the suddenly interrupted person may collapse. For example,
�anger� may collapse through �confusion� to �frustration� to �brooding� till
the dramatic theatre unfolding around them �captures� their attention and they
shift to being profoundly engaged as part of the audience to other�s
change-work.
An
Example of Ecology Therapy
The �never take sides and support the ecological bits of all
concerned� framework of ecology therapy may generate very subtle strategies.
For example, a very talented woman with major psychological difficulties was
avoiding doing healing work on herself by using her considerable administrative
skills within a number of the patient committees. She had so mobilized the
women patients to assist her on the committees that the gender balance was in
Neville�s terms, �out of whack�. The women patients were according to Neville,
�running the show�. The other patients had recognized that this �excessive
involvement� by this woman was avoidance behavior in respect of her own
healing.
At Big Group, Neville thanked the women for all the obvious good
work that they were doing and berated the men for not pulling their weight in
committees, and before any male could respond Neville asked for the women�s support
in using their considerable administrative ability to get the men involved so
that gender balance in committee work could be re-established. The women
accepted this challenge and in a very short time gender balance was restored.
The women on the committees worked on the woman talented in
committee work suggesting that she be one of those who make way for increased
male involvement so she could get on with her own change work. This woman bowed
to group pressure and relinquished all her roles and did get on with her own
change-work. Neville here used recognition of the ecological parts of the women
to have them lower their power. If he had confronted them about their excessive
use of power, it is highly likely he would have met their resistance to their
relinquishing power, and in forcing gender balance, he could have easily
created aggrieved �losers�. The men, for their part welcomed the return to
gender balance. This interaction is another example of �doing the opposite of
the obvious�, namely, co-opting the talent of the women and giving the men a
�rev up�. It is also an example of working with the free energy in the total
group. It was the woman patients, not the staff, who engaged in mutual help in
supporting the talented woman getting on with her change-work. The process was
self-organizing. They engaged in mutual-help and self-help. It was Neville who
set up this possibility.
The
Flexible Enabler - Control and Abandon � Surrender and Catch
As leader, two of the roles Neville used
were �enabler� and �orchestrator�. For this, Neville was accused of being
irresponsible and not doing his job of leading - loosely defined as, �telling
everyone what to do�. Being the Director and Psychiatrist in charge of the
Unit, he was expected to do just that. In his profound love of all involved,
Neville was accused of being, �too emotionally close�. In his tight, tough,
humane, meticulously specific, and precise interventions in crisis contexts he
was accused of being a megalomaniac. Accusations would depend on which moment a
critic happened to be observing. The seeming conflicting roles of
non-interventionist/interventionist and uninvolved passive/totally involved
tyrannical megalomaniac are fully consistent with use of opposites and
cleavered unities. Neville�s behavior was consistent with his behavior being
superbly appropriate to each passing moment and context.
There is
another sense in which Neville used control and abandon in his own functioning.
It is resonant with what Castaneda�s wrote about the Yaqui Indian, Don Juan�s
way. Don Juan spoke of walking the path between control and abandon and how to
combine both of these in peak performing - to control oneself and at the same
time abandon oneself. � to calculate everything strategically - that�s control,
then once this is done, to act, to let go; that�s abandon (Castaneda
1974). Neville
could seamlessly slip between control and abandon or use both simultaneously at
differing levels of functioning. This letting go and abandoning is resonant
with Wolff�s writings in his book, �Surrender and Catch� (Wolff
1976). Even in
surrendering/abandoning there is keen seeing of what others may not see.
Neville used and fostered
�practical healing wisdom in action�. Neville knew of the Rataiku people of
Bougainville who have the word �Haharusingo� for �loving wisdom in action� (Misang
1998). For Neville, practical
wisdom was always linked to place and context and embodied, especially
emotional- kinesthetically, and was linked to all forms of artistic expression (Yeomans and Spencer
1993). The person of
practical wisdom deliberates about things that are variable, not about things
that are invariable or impossible. Neville describes a pervasive passive
feeling as the source of the passive voice form in the language he typically
used.
As for Neville�s view on drug
based therapy, licit Drugs were used, but as a �last option�. In Fraser House
there was no drug-induced oblivion for containment as occurred in the back
wards. The head charge nurse/sister was authorized by Neville to sedate
patients, and quite prepared to do so if they were a definite danger to
themselves and/or others and the timing and circumstances warranted it rather
than using other more preferred interrupt strategies. Stephanie Yeomans said
that in her experience there was no culture of illicit drugs use in Fraser
House and this would not have been permitted by Neville.
Differing
Patterns of Interaction
To get a sense of Neville�s (and his father�s) phenomenology,
think about de Bono�s types of thinking. Imagine refining divergent thinking so
that everything is linked to everything, and then tempering this with thinking
filters � like, �look for free energy�, �look for emergent properties�, �look
for the patterns that connect�, �look for what works close to what does not
work - where there may be potential for a ripple through effect�; and then
going into serendipity and creative thinking, and blending this with strategic
thinking of the, �what if�, and �if this then x.y.z��, and then further linking
this to a �devils advocate� or �what could go wrong� type thinking, and then
imagining all of this psycho-physical-verbal-emotional internal action
happening in nanoseconds; where (as in Fraser House) Neville experiences
something happening the moment he walks into the room. He then
�instantaneously� responds superbly to stop a potential murder! This incident is
discussed Chapter Six.
Neville had noticed that there was a differing pattern to group
interaction according to size (Yeomans 1965, Vol. 5, p. 64). Groups below twenty may be intimate. Attendance of between
twenty to fifty people tended to have a pattern emerging in the interaction
that takes the form of the discussion leader giving little lectures or sermons
or taking on a teacher role. This discussion leader role may shift between the
designated group leader and other staff and patients. Once there were over 50
people shoulder-to-shoulder, those present became �a crowd� with a different
dynamic, where crowd stimmung, synchrony and contagion were possible for
collective affect. Because of the above observation, Neville kept groups under
twenty or over fifty.
Neville was particularly
interested in processes for crowd synchrony and contagion and how to use this
for enabling caring and wellbeing. Neville�s models for his own Big Group
leader behavior were Churchill, Hitler, Billy Graham and Jesus - that is,
people who could create crowd synchrony and contagion; people who could
inspire, manipulate, emotionally move and control a crowd. He did not use them
as content models. He often mentioned to staff and clients that he used these
charismatic people as process models.
Delivering
Miracles
Neville�s abiding
metaframe was love surrounded by humane caring, psychosocial ecology, and
safety. Aspects of this metaframe emerge through this research. In a 30 June 1999
conversation Neville said that one appeal of charismatic leaders is that, �for
many followers, the paradox of existence requires the intervention of the
miraculous. Many believe that such leaders can deliver miracles�.� When I said, �And there were miracles at
Fraser House�, he said with flourish, �Of course it was miraculous. We were the
best in the planet, and we all believed this, so we would acknowledge our
failings, as we were streets ahead of
everyone else. I was accused of being an impossible optimist. I sense I was
more of a fatalistic optimist. I didn�t know then that the system was falling
apart.� I was context driven - if I go to
�creative context� then �everything is creative� - it worked like that. As for
the miraculous - well that was a calm night.....peaceful.... remember we were
filled with the very bad and the very mad - the under controlled and the over
controlled.�
Neville�s
Sensory Functioning
According to Bruen and
Chilmaid in April 1999 Neville had an amazing ability to perceive inside and
outside of the person(s) he is attending to, as well as every person in the
group (up to 300), and to do all this instantly, and be ten or more steps ahead
of everybody in a very strategic way. Neville had the capacity to
recall virtually verbatim everything everyone said and his or her non-verbals
and actions over at least the whole of a one-hour Big Group (around 180 people)
or small therapy group at Fraser House. Often he would refer a person back to
what they had said 20 or 40 minutes ago and be able to repeat verbatim what
they said back to them.
It seems that in sensory terms, when Neville was tuned into social
interaction, he typically stayed attending to external as opposed to internal
recalling or imagining seeing and hearing things. He would receive thoughts as
guides to action as �bolts out of the blue� � out of internal silence � with
these, and their link to unfolding action, linked to his immediate (fast)
emotional and kinesthetic responses as a check on ecology and �fit�. He could attend
to specifics and scan the context concurrently, always looking for the free
energy in the social milieu. For Neville �free energy� was the context specific
and resonant functional bits of behavior and the psychosocial resources in each
person present. This theme is discussed more fully in Chapter Six.
Place was fundamental for Neville. Initially I had not realized
that when he and I were talking about another place (or events in another
place) to the place we were situated, Neville would mentally place himself in
this other place as an aid to discussion and functioning. Similarly, Neville
always checked out his and others� context and metacontext (the context of the
context) in social exchange, so that he could get a feel for the interconnections in everyone present (Goffman 1974). None of this detail ever bogged him down or cluttered the
conversation. Neville was a man of few words � for him, the less said the
better.
On
Going Berserk
Four major themes stirring emotions are gain, loss, threat and
frustration. A discussion of neuro-psycho-biology underlying these states and
the relationship between the therapeutic processes used by Neville and internal
functioning is discussed in Chapter Six. Neville would expressly use incidents
with a high probability of heightening emotional arousal within Big Group.
Below is an example of how Neville intentionally heightened the group�s
emotional arousal during a Big Group meeting.
On one occasion after Fraser House had been going for around two
years, and as soon as Big Group started, Neville went berserk. All present
thought Neville was having a mental breakdown. At first, Neville was just
screaming and yelling. Then he conveyed that he was sick of everything. This
raised everyone�s� emotions. Threat was a dominant theme. After a short time
the nub of Neville�s outburst was revealed. He was going on extended leave and
the Department had not arranged a replacement. This was a serious matter.
Neville�s (Yeomans 1965, Vol. 5, p. 1-14) file note at the time about going berserk in Big Group� said in
part:
�With my impending holiday
today I allowed my aggressive frustration full play in the community meeting
this morning. The meeting began by John asking me if I was really going on
holidays. I said I was even if the bloody place fell down. I then berated the
Division and the fact that Dr ----- or some other Doctor should have been here
at least two weeks ago.
I took a most regressed
and childish aggressive view against the department and in support of Dr
Barclay (head of North Ryde Hospital) and my own efforts, pointing out that
both of us were letting them down because of the department�s incompetence.�
Neville�s outburst had made �threat and anger through loss�, a
dominant community focus. The Unit would be without a doctor/psychiatrist. Some
replacement was coming in two or three weeks, but in the meantime, they were
�on their own�. Even when the replacement got there, he or she would have no experience of �the Fraser House� way.
There was the major uncertainty of what changes a new psychiatrist would make
in Neville�s absence. Neville was scheduled to be away for many months.
Neville�s behavior and this news heightened emotional arousal to fever pitch in
everyone - a combination of anger, rejection, abandonment, confusion, anxiety,
panic, frustration and fear. Neville then slammed the Department as the
�culprit�.
Both patients and staff�s emotions were, by this shift in focus,
directed into anger at the Department. Then Neville refocused thinking to
�everyone taking responsibility for Fraser House and each other�. Again,
patient and staff emotions were directed into this new issue � of �self-help
and mutual-help�; another mixture of emotional energy - panic, concern,
uncertainty, questions of being up to the task, to name a few. Then Neville
drew everyone�s attention to the suicidal nature of one of the patients present
in the room and laid it on the line that this person�s wellbeing - his very
life - was in everyone�s hands. This was the next shift in emotional focus.
Here the focus was on gain in the face of loss and threat, and how to get gain
safely. Neville�s interaction with staff and patients was all about engendering
communal cooperation towards safety and gain in the face of danger and loss.
Neville arranged for eight separate people�s reports of the
particular Big Group meeting where he went berserk to be placed in the archives
at the Mitchell Library (Yeomans 1965, Vol. 5, p. 1-14).
�Everyone of these reports
similarly confirmed that Neville had intentionally mobilized and used group
emotional energy towards group cohesiveness in caring for itself, and that this
shifting around of emotional contagion was a crucial aspect of the Unit
functioning extremely well during the ensuing months (nine) while Neville was
on holidays. One staff member�s report of the above incident ended with, �This
story has no end because we still continue to function as a unit� (Yeomans 1965, Vol. 12, p. 2). Another staff member wrote a file note saying, �I have no vivid
recollections of the first week of Dr. Yeomans absence except that the nursing
staff occasionally seemed surprised that the ward was still running and that we
were able to get through staff meetings without Dr. Yeomans� (Yeomans 1965, Vol. 5, p. 15). Warwick Bruen in April 1999 also recalled Neville�s behavior in
going berserk in Big Group and collaborated the above material.
Placing eight separate staff member�s reports along with his own
report of the �going berserk� incident and its sequalae for me and others to
find in his archives is another example of Neville, �the researcher strategist
par excellence�. I suspect that he did this expressly for the likes of me to
find them all nearly 40 years on!
Phil Chilmaid mentioned one Fraser House research project that
demonstrated that there was a consistent pattern that significant
�break-throughs� tended to follow about 6-7 days after some major crisis (Cockett and Chilmaid 1965).
Neville
as Dichter and Denken
Recall that in the methods section in
Chapter Two in writing about Dichter and Denken (Pelz 1974) I said, �In the Fraser House outreachings
and Laceweb networking contexts, we may contemplate the merging of firstly,
Neville and his other system designers/co-reconstitutors, secondly, system
designing/co-reconstituting, and thirdly, the system(s); and in so doing,
perceiving these three as a connexity/holon�. An example of Neville�s use of
Dichter and Denken in Big Group and other contexts was his simultaneously
scanning for initiators of, the initiating process involved in, and the
unfolding of, gain, loss, safety, and danger and the interplay of high/low
levels of each in patients, outpatients and staff - e.g., safely doing
dangerous things, while maximizing gain and minimizing loss; another is
spotting when relatively safe things are being done dangerously for little gain
and potential for high loss. In all this Neville is using non-linear
multi-sensing processing. Here I am talking about 'connexity perception'. A
part of this in the visual sense is simultaneously attending to visual full
field - the ever shifting background-foreground distinction, the flitting point
of high acuity, the distant-close distinction and the peripheral; and including
in awareness the aware self as responding perceiving (sense-making)
mindbody-viewer, the viewing and the viewed. In the July 2000 Gatherings in
Cairns discussed in Chapter Nine the Brazilian enabler had participants experience
micro-experiences for increasing �connexity perception� (Laceweb-Homepage 2001). I enabled participants use these
micro-experiences in workshops during the New Year ConFest in January 2001
Big group was a potent context for emotional corrective experience.
To reiterate, four major themes stirring emotions are gain, loss, threat and
frustration. Another simple model with similar focus used by Neville involved
two continuums set along the X and Y axis, namely safety-danger and gain-loss (Clark and Yeomans 1969, p. 17). This is depicted in Diagram 08.
Diagram
4 Neville�s Model
Most of the criminality
group had no sense of danger or when they were in dangerous situations.
Typically, they also had no sense of contexts wherein safety and loss were
issues. Normal people tend to have �alarm bells ring� (or something similar)
when they sense danger. For example, seeing someone about to plunge a live
electrical appliance into water will typically galvanize action. �Stop!! Don�t
do that!!�
�Typically, people who end up in jail may have
some notion of gain or payoff with no awareness in the other quadrants. If they
have the thrill of danger, this is not balanced by an ecological sense of
safety and potential for loss. Over-controlled, under-active people may be
obsessed with safety or loss, or both of these, and have little sense of the
danger involved in these obsessions. They may have little sense of how they may
take action towards gain or a more balanced ecological sense of safety. Neville
would have the above model as one of his aids to understanding and action.
Nanotherapy
One Fraser House process
Neville called nanotherapy, where �nano� means a 1,000 millionth part. He
likened it to precise micro detective work - focusing on the tiniest bits of
verbal or non-verbal behavior. Something trivial may be mentioned or conveyed
non-verbally and this may be picked up and explored in minute detail. Newcomers
would typically become bored or annoyed by this preoccupation with minutia.
They soon learned that the exploring of minutia invariable led to major
breakthroughs for the focal client(s) and that this in turn rippled through to
change others who were seemingly uninvolved. By modeling Neville�s nanotherapy,
both staff and clients began using it as an integral aspect of their relating.
In the Big Group nothing
was taboo. The Sixties were far more prudish than now, and yet in the Big Group
anything could be discussed. On one
occasion there was a detailed discussion of a patient who was obsessed with
painting his scrotum blue. Neville told me of this scrotum incident in 1993. It
was confirmed by Chilmaid and Bruen in April 1999. During the early part of a
Big Group, Neville kept engaging this patient about his blue scrotum - on and
on ad tedium. After forty minutes of the patient�s constructive struggling had
been enabled, acknowledged and respected by Neville, it became apparent to
those present that all manner of people were beginning the resolving of aspects
of their own ambivalence, conflict and confusion about their own sexuality and
relating with others. The blue scrotum became the catalyst for community
loosening up. One by one patients and outpatients started disclosing aspects of
their sexual life that they could see as �somehow related� to this other fellow
and hence, in this place, safe to discuss.
Cliques,
Factions and Use of Space
While the rotating of
patients as well as their friends and family members through various small
groups tended to cleaver pathological groups in functional ways, typically
people could sit where they wanted in Big Group. Cliques and factions would be
continually forming and disintegrating within Fraser House. This would be
particularly evident in �who is sitting beside whom, and where� at Big Group.
Community processes would constantly contribute to disintegrating unhealthy
factions - not to remove factions - rather, to enable the forming of healthy
factions (from Neville, April 1999). As well, some patients would become for a
time, �isolates� (From Chilmaid, April 1999s�; also refer Clark, A. W. and
Yeomans, N., 1969, page 131). Occasionally people would be separated by staff
or patients if they were causing intolerable disruption.
A particular spontaneous
pattern to the use of space in Big Group was recognized by Neville. This is
depicted in Diagram 07.
Clients who saw themselves
as Neville�s administrative faction (constructive administrative) would sit
beside him on his right. Emotional supporters (constructive emotional faction)
would sit beside him on his immediate left. Further on the left would be the
emotional destructive faction. Further on the right would be the administrative
destructive faction or utilitarian rationalist faction. On the far left would
be the mad. On the far right would be the criminal/bad (from Neville, April
1999). Since Neville pointed out this use of space by factions, I to have
frequently found this same use of space by the same factional groups (in
relation to a key figure in the group) in my own group work. Recall that in
medieval times, the Kings �right-hand man� - the Kings Champion - would sit on
his right hand side.
This spontaneous use of
space in Big Group has fractal and connexity aspects as well as hints of
embodiment and mindbody effecting individual and group behavior and vice versa.
The left-right cleavage and behavior characteristics as an aspect of space
choice approximate the split in brain hemisphere function. The right hand side
of the body is controlled by the left hemisphere where linear, rational
logically processing occurs. The liver (for energy) is on the right-hand side.
Many of the fight flight ergotrophic functioning (refer Chapter Six) is on the
right hand side of body with left hemisphere involvement. Note the active
constructive/destructive administrative and the active mad sat on the right �
the in-your-face active who, while often emotional are typically dissociated
from emotion. The left hand side of the body - the hearts home � has links to
right hemisphere functioning with holistic and artistic aspects. The emotional
constructive and destructive as well as the disintegrated mad were
spontaneously on the left. A lot of their attention is internal and responding
to emotion. Note how all of this is reflected in the spontaneous use of space
in response to the �power� spot of the Big Group Leader Facilitator.
Diagram 5 The use of space in Big Group
The four corner positions
were also trouble spots and were typically taken by troublemakers, nudgers and
whisperers. Neville wrote a paper on this called, �Whispers� Relationships � A
Collusive Alliance� (Yeomans 1965, Vol. 5, p.
38). Neville, in speaking of
the constructive emotional and the constructive administrative support in a
paper entitled �A General Theory of Welfare Functions� included the following
Table 04 (Yeomans 1965, Vol. 2, p.
38 - 40.).
Recall that Neville
engaged both forms of opinion and action leaders among patients and staff for
support in sustaining the two functional imperatives, (a) serving to maintain the stability
of the system and (b) maintaining the interaction of the system as a system
with other systems within systems. Neville and Margaret Cockett research into
different forms of leading is discussed later in this Chapter.
|
Integrative
role of Emotional Leader Affectional
� Integrative primacy Subjective
component: ��� Prestige ������� Friendly � Unfriendly ������� Pleasant � Unpleasant |
Administrative or
Instrumental Instrumental Primacy Subjective
component: ���
Respect �������
Weak - Strong |
Figure 1 Constructive Emotional and Constructive
Administrative Support
Once when the far right
criminal/bad Mafia faction were really blocking progress in the group, Neville
ruined their sabotage by being in Neville�s terms, the �angel of God under
their bums�. They were all sitting on a raised section at the back of the room
and Neville had someone who was skilled at the task, take over chairing the Big
Group meeting and he, with the Mafia�s knowledge, went and crawled in
underneath where they were sitting. In some �magical way� this totally
interrupted their behavior and a number of things that had a very long history
of pathology were quickly resolved. This is an example of Neville�s recognition
and use of significant space and place.
Functionally
Mingling Dysfunction
Some professionals hold to
the view that people with certain mental disorders should not be in group
therapy. Neville challenged this. �We
mingled all manner of disturbed people every hour, everyday. In a conversation
with Neville on 30 June 1999 he said, �Sure, things happened, though nothing we
couldn�t handle.� Some peers claimed that group therapy for schizophrenics
would definitely make them worse. Neville found that he got excellent results.
He found that he got even better results when there were criminals in the
therapy group with schizophrenics. Schizophrenics often have difficulties living in their pathological social networks.
Many of the criminals had learnt, albeit in anti-social ways, how to live amongst social pathology. They had
no compunction about making withering remarks to the domineering mothers of
over-controlled underactives. Neville said that it often happened that
schizophrenic patients who were overwhelmed by their pathological parents and
in a helpless hopeless state would see their polar opposite (under-controlled
over-active) suddenly reducing their �all-powerful� parents to metaphorical
ash! �They�re nothing!� Time and again, anxious, tentative over-controlled
schizophrenics would be amazed at the under-controlled criminals� approach to
things that they found overwhelming. Where a Schizophrenic may tremulously
say,� �You can�t do that, their criminal
room mate may reply,� �Oh yeah! Just
watch me!�� Often seeing a fellow patient
put their parent firmly back in their place was a life changing experience for
the over-controlled under-actives. Neville�s comment on this was, �No one is totally under-controlled or totally over-controlled. Both the
�schizophrenics� and the criminals moved to the center - to being more
functionally normal.
One therapeutic aspect of
the above exchange is the denial of the schizophrenic�s reality (Hanlon 1987) - namely that something was �not allowed� or �not possible�. The
criminal sets up a new frame (Goffman 1974) - a world where �being allowed� is irrelevant, and something
being �necessary� is just not so and
instead something is possible.
When the criminal does do
what he said he would do, the �schizophrenic� may see the consequences �
namely, their supposedly all-powerful parent retreats. Within Fraser House�s
controlled environment, the forceful confrontation of the domineering person
typically would neither bring the end of the World nor disastrous consequences.
Clark and Yeomans refer to a similar incident to the above
criminal rejoinder (Clark and Yeomans 1969).
This time it is the over-controlled who is experimenting with
using assertive rejoinders:
�The group not only
encourages and supports new behaviors, but provides patterns on which it may be
modeled. Thus it can be seen in the following exchange how an under-controlled
patient, Barry, aged 20, both provoked John and provided a model on which he
could base aggressive behavior: Barry, �Oh, why don�t you shut up?� To which
John replied, �Why don�t you should up?�
Most importantly it was
only within the shelter of the group that John was courageous enough to use
such an aggressive rejoinder. It was here that he saw under-controlled patients
behaving in this way without catastrophic results and, that at the same time,
knew that he would be protected against actual physical assault, of which he
was usually terrified.�
This
is another example of a trivial exchange/action, which in context has immense
transformative potential.
Labeling
Neville well knew the potency of
labeling, especially the potency of using terms like �patient� and �mental
asylum� in constituting and reifying aspects of people�s response to
themselves, each other, and their place in the world. On the issue of labeling,
Neville preferred the term �resident� rather than �patient�. However, in his
words, �Not to use �patient� was just too hard within the hospital milieu at
the time�. All patients who arrived at Fraser House already arrived with a life history of negative labeling as
psychosocial baggage that they had to live with. In Neville and the
interviewees� view, the combined Fraser House process easily outweighed the
effect of all this negative labeling.
SOCIAL
CATEGORY BASED SMALL GROUP THERAPY
The Small Groups were
mainly conducted by the nurses, with some groups being lead by medical
officers, the social worker, and the chaplain. Margaret Mead ran a Small Group
when she visited Fraser House. The chaplain ran some spiritual groups.
Typically, one staff person ran the Small Group and one other staff person was
a process observer, on-sider and trainee. Just like Big Group, Small Groups
were run like meetings. The Fraser House Handbook written by patients specifies
the nurse therapist role in Small Groups:
�The role of the Small Group therapist
and observer has always been the province of the nurse in Fraser House, and
represents part of the rise in therapeutic status. Nurses have become
therapists in their own right.
The first essential in taking
a group is to see it as a meeting, and like all meetings, there is a need for a
chairman to conduct affairs and keep issues to the point.
�The initial function of the therapist is to
see that the group functions as a group (Yeomans 1965, Vol. 24 p. 18)�.
The Handbook then gives detailed
specifying of group process. Sections of the Handbook on the Nurses Roles and
Big Group process is Appendices 4 & 5.
Small groups were held
from 11 A.M. to 12 Noon and were preceded by a staff discussion over morning
tea reviewing the previous Big Group meeting. After a similar Thirty-minute
staff discussion period, Small Groups were run from 8 p.m. to 9 p.m. During the
staff discussion, patients and visitors had an informal morning tea together
separate from the staff. All groups and the refreshment break ran strictly to
time. To reiterate, this was to prevent what Neville called, �session creep�.
Generally, nearly all the outpatients
(typically, friends, workmates and relatives of patients) attending Big Group
stayed and were allocated to the various Small Groups in both the morning and
evening sessions. It was expected that outpatients attend both Big and Small
Groups. There were ten or more concurrent small groups typically made up of
between 9 to 18 people, or more per group

Drawing 1 A Sketch of a Fraser House Small Group
Small Groups were formed
of people having common bonds based on common sociological categories. Each of these
categories was as important a factor in socio-therapy as they are in sociology
theory and wider society. All the groups at any one time were of the
same category. The social categories were: (i) age, (ii) married/single status,
(iii) locality, (iv) kinship, (v) social order (manual, clerical, or
semi-professional/ professional) and (vi) age and sex. Friday�s Small Groups
were made up according to both age and sex for both staff and patients. This
was the one exception to the non-segregation policy. Often inter-generational
issues, including sexual abuse issues, were the focus of these Friday groups.
Both the sociological category and the composition of Small Groups varied
daily. People in pathological social networks would be all together with everyone
else in Big Group. However, because of the continual changing
composition in Small Groups, the members of these pathological networks were
regularly split up (cleavered) for the Small Group sessions. Age grading was
deemed very important, as it is one of the basic divisions in society. The
thinking was that age grading sets a context for the production of personality
changes to prepare the client for normal outside life. Age grading also allowed
space for sorting out inter-generation pathology that was very prevalent.
Because of the number of
categories, any visitor coming regularly on certain days of the week would find
that they would be attending groups based on differing categories. For the Small
Groups based on locality, Sydney was divided into a number of regions. In most
cases, groups of people came regularly on the same trains, buses and each
other�s cars so they all got to know each other. Patients and Outpatients would
attend the Small Groups allocated by locality for their region of normal
domicile, and typically, by the time they were about to leave, they would have
formed a larger friendship/support network of around seventy people.� This meant that people who may have
previously had a social network that was smaller than typical in society, ended
up having one that was typically larger in terms of the number of people in the
�closely known and regularly interacting� part of their social network. These
individual patient family/friendship networks would have members with
cross-links to other patient�s networks, and with a continual changing Unit
population with overlap in stays, these nested patient-networks became very
extensive. As well, all these people had all of their rich Fraser House
experience in common, and a common set of advanced communication and mutual
support skills. The critical role of locality and Neville�s use of locality in
this increase in the size and functionality of patient�s social networks is
entirely resonant with Indigenous links to place and the significance of place
and placeform in Keyline. Recall that Neville used to say that he wanted to
increase locality, meaning �people connecting to place�.
PARENT
PLAYGROUPS
Large and small
child-parent groups were held on Tuesday nights where attendance was based on
being a parent with accompanying child. Therapeutic play relationships were the
primary focus for the first half. Typically, parents were extremely reluctant
to play with their children when they first started attending. The first
segment involved parents and children interacting. Often these became very
emotional with many parents demonstrating poor parenting and coping skills.
During the second half, the parents remained in the same room, and the parents
together with staff enablers would process the interaction that had happened.
The children went upstairs and continued play. Terry O�Neill used to facilitate
this upstairs child-play segment as a volunteer psychologist when this Parent
Child group first started in the Sixties. You may recall that I received my
counseling skills training from Terry in the late Seventies. He told me that on
his first evening alone with the children, so much emotional energy had been
generated during the first segment, �playing� with their parents, that the
nature of the frenzied play upstairs was scary. Some of the older children were
kicking a soccer ball round like a deadly missile. Everyone had to be super
alert not to get his or her head knocked off. Terry said that having a number
of disturbed children in play therapy in these evening sessions stretched his
skills to their limit.
After having the Fraser
House experience for a time, Terry came to Melbourne to take up a counseling
role and joined a self-help group of psychology/counseling professionals who
met regularly. Terry stated that he was assimilating, making sense of, and
adapting into his counseling work the Ways he learnt from Neville and Fraser
House for many months after arriving in Melbourne. When I interviewed Terry in
the late Nineties he said that in his subsequent counseling work he would often
mentally return to his Fraser House experience as a guide to action.
INDIVIDUAL
THERAPY
When deemed appropriate to
connexity, face-to-face therapy between two patients, a patient and a nurse, or
a patient and a doctor was held regularly. Even in this individual therapy, the
central focus was inter-patient relationships. Encouragement was continual
given to �bring it up in the group�.
While it was recognized
that during some crisis times, individual support was needed by a doctor or
nurse, most face-to-face therapy was between patient and patient, with the
wider community always a background.
DOMICILIARY
CARE
Fraser House pioneered
home visits and domiciliary care by psychiatric nurses and patients. A monograph reports that follow-up
groups to homes became routine in 1962. (Yeomans 1965, Vol. 4. p. 2-4). Patients,
who had substantially changed to being psychosocially functional and proficient
as co-therapists and were anticipating leaving the hospital themselves in a few
months, would call on ex-patients and their families and friends to assist and
resolve difficulties (Yeomans 1965, Vol. 5, p.
63). Neville wrote that these patients
involved in domiciliary care work were very skilled and helped �to destroy the
lunatic image that often some of these disturbed relatives have of the hospital
and other patients in it (Yeomans 1965, Vol 5, p. 106).� Participating
in Domiciliary Care was not time based - �so many months prior to leaving� -
rather �psychosocial health and competency� based.� This use of patients who had not been
released to support those who have, is resonant in some aspects with de Bono�s
lateral solution to ensure that a potentially polluting industry that requires
clean water itself remains environmentally responsible - require it to
discharge its water upstream of its own plant water intake. Fraser House,
patients were helping ex-patients settle back into the community before they became ex-patients
themselves.
Upon reading my juxtaposing the De
Bono example with Fraser House, a colleague of mine Dr. Dihan Wijewickrama wrote,
��the two processes are not strictly isomorphic. In fact one is an example of a
first order cybernetic system - imposing control on a system - steering it so
that it establishes a normative behavior. The process is essentially a
corrective process and appears to have a ceiling to the benefit. Fraser House
was a second order cybernetic system - potentially self-steering. The
process here is self-referencing (positive feedback) and reconstituting -
current patients helping ex-patients to fit better into community reconstitutes
everyone double dividends. There would probably be no absolute ceiling to the
benefits - community making more and more wellbeing both inside and outside
Fraser House. Wijewickrama has written on second order cybernetics (Wijewickrama 2001).�
Aspects of this
domiciliary care have been adopted into mental health practice with staff doing
the visits. An early example modeled on Fraser House was the Domiciliary Care
Program at Kenmore Mental Hospital in Goulburn (Mitchell 1964).
The little red van used
for this domiciliary care, including petrol and maintenance costs, were funded
and maintained by the patients through the profits generated by their Fraser
House canteen. A group of patients would often go, without staff, on these domiciliary
visits. The Follow-up Committee would also be continually requesting the
visitors, relatives and friends for patients to be able to use their cars and
petrol to conduct domiciliary visits (Yeomans 1965, Vol. 5, p.
63). After a time it was
decided to keep activity records and during the first nine weeks of activity
recording (1 July 1963 to 6 Sept 1963) there were 71 group activities to homes.
The average was just under 8 visits per week with a range of 5 to 12 per week.
SUICIDE
SUPPORT PROCESS
From the outset of Fraser House a
Suicide Clinic was set up as an aspect of the Unit. This may have be an
Australian first. Neville obtained a lot of media attention about the role of
this Clinic. In 1959 the Weekender reporter Green tells of a dedicated
telephone number for Fraser House being SUI, similar to 011 today (Green
1959); telephones in those
days had alpha and numeric numbers. People at risk
and their family and friends could attend Fraser House as outpatients and at
risk people could become inpatients. After only four months in operation,
Fraser House had a five-month waiting list of people wanting to get in.
Neville was constantly seeking and gaining
media attention on Fraser House. Neville placed a large collection of media
clippings and other Fraser House archival material in the Mitchell Library
within the NSW State Library (Yeomans 1965). Within the first nine months, Fraser
House had hundreds of calls on their suicide hotline as reported in the Sun
Newspaper, June 23 1960 (von Sommers 1960). Other Newspaper articles had
headings like �Suicide Urge � Clinic Saves Lives� - The Neurotic and
Alcohol Unit of the New Psychiatric Center at North Ryde� (1960), �Pulled
From the Brink Suicide Clinic� (1960), �Dial the
Club and Talk it Over � Men Who Stop Suicides� (von
Sommers 1960), �Alcoholics
V Neurotics� (1960), �880281 � A
Phone Number That Saves Lives� (Kelly
1962),
and �Why do People Commit Suicide� (1962). The Readers
Digest ran a story called, �Love From a Stranger� in May 1960 (1960). The Pix
Magazine ran a special report on 14 October 1961 called, �Are You a Potential
Suicide� (1961).
In evolving support for
suicidal people Fraser House adopted the process of having patients and staff
constantly around potential suiciders as a support and crisis intervention
group so that suicidal people were never
left alone. Patients would be co-opted as therapeutic enablers and patients
could and did take on the role of being caring support for other patients,
especially those in danger of self-harm. Any person who was in a heightened
emotional state, disturbed or suicidal would be immediately �specialed�. This
meant that two patients or a patient and a staff member would continually stay
with that person (and be replaced by another shift if necessary) until, on the
say of a group, the �specialed� status was removed. Processes were set up such
that a cooperating team of patients
with or without staff would take on the responsibility of providing twenty-four
hour support to other patients at-risk of suiciding, and in the process gain
response ability. In the archives there is only reference to one suicide at the
unit. Neville and three other staff people I interviewed confirmed that suicide
was extremely rare in Fraser House. Patient suicide was common in other
hospitals.
Recall that when Neville went
berserk at the start of Big Group when he was about to take leave, Neville
harnessed group consternation around him taking leave without the health
department arranging a replacement, to galvanize support around a suicidal
patient. This idea of setting up support processes for suicidals was
subsequently used elsewhere in the wider society and became a standard practice
in mental health services. However, outside of Fraser House, I understand only
staff are used in the support process. Previously, the practice had been to
isolate suicidals and keep them under periodic observation. However, this
practice may be inadequate - it only takes a few minutes to choke to
death!� In Fraser House �Special Groups�
could be called at any time whenever a crisis occurred. These groups would last
as long as required to �do the job�.�
Fraser
House may well have been the primary source of Australia�s suicide telephone
help lines. Neville had started to give a constant stream of talks to churches
and other agencies as part of his linking of Fraser House into the community.
Fraser House became known in Sydney as the place to call for suicide support.
Requests for help with potential suiciders came from all over Sydney. Often
patients alone or with nurses would go from North Ryde over to the Gap at all
hours of the day and night to talk suicidals into come off the edge. This
having patients seeing their Fraser House therapeutic community having wider
community relevance, and seeing their own healing ways and their peers as significant
to themselves and others, was yet another element of the Fraser House healing
process. Photo 24 shows how far North of the city Fraser House was. Patients
would have to go into the city and then on to the Gap on South Head. The Gap
has very high cliffs looking out on the Pacific. This makes rescue and crisis
counseling all the more precarious and potentially life threatening for the
counselor(s). Even if a person decided to return to safety, they could be so
distressed, the climb back may be dangerous, especially in rainy and windy
weather.

Photo 2 The Gap at South Head

Photo 3 The Sheer Cliffs at the Gap
Neville began speaking at Ted
Noff�s Wayside Chapel at Kings Cross in Sydney and at other places. Neville
mentioned to Noff that Fraser House could not carry traveling the distance between the North Ryde and the public
calls Fraser House was receiving about helping potential suiciders. Neville
invited the churches and other agencies to take over the suicide help line. The
Wayside Chapel started a helpline. The telephone emergency service �Lifeline� was set up by the Methodist Central Mission
in Sydney in 1963 (Bootes 1978).� This evolving of
telephone emergency services was confirmed by Neville and Bruen in April 1999.

Photo 4 Photo of the city skyline from Fraser House as
indication of distance. This photo also indicates the convex to concave
Keyline
RESEARCH
AS THERAPY
Neville commenced his postgraduate diploma
in sociology shortly after Fraser House started, and completed it in 1963. He
spoke of Fraser House being, in part like a Post Graduate Research Institute
and of the Unit being the most advanced Social Research Institute in Australia.
Neville had pointed out to
me that Franz Alexander had observed the potential for healing of the caring
relationship between Freudian analysts and patients (Alexander 1961). Similarly, Elton Mayo (Trahair 1984) had found in the Hawthorne experiments amongst workers in the
early part of this century, that the change component was not so much the
various �treatments� of the research - rather that it was that the researchers
were acknowledging the workers� dignity and worth and showing an interest in
them. Change was linked to the emotional experience of being research subjects.
Similarly to Mayo�s work,
Fraser House patients and staff were the focus of continual research by Fraser
House researchers and the outside research team headed up by Alfred Clark.
Patients were being continually asked to reflect on themselves, other patients,
other staff, Big Groups, small groups and on every aspect of Fraser House and
aspects of wider society. Fraser House staff were totally devoted to patients�
healing, and patients experienced this emotionally on a daily basis. Through
all of the research, patients learned about the notions of� �validity�, �reliability testing� and
�trustworthiness�, and how these are very useful notions as part of living in a
modern community, especially one riddled with pathology. Patients also became
involved in both qualitative and quantitative research data gathering and
discussion concerning the results of research.
During 1963-1966 research by nurses in
Male wards in Fraser House was supervised by Neville (Yeomans 1965, Vol. 12, p. 69). Neville gave preliminary training of
nurses in research methods and also trained the social worker in research
methods. At one time Neville arranged a Fraser House Research workshop with 25
associated projects (Yeomans 1965, Vol. 12, p. 86-99). One
example was a consensual technique that involved patients considering the extent
of patient participation and improvement. Patients were asked to nominate which
patients were the �most� and �least� in various categories for questions like
those in Figure 05:
�
Who are most involved in therapy sessions?
�
Who are least involved in therapy sessions?
�
Who think that being in the Unit is least worthwhile for them?
�
Who think that being in the Unit is most worthwhile for them?
�
Who get on well most with staff?
�
Who get on well least with staff?
�
Who join in least on social and recreational activities?
�
Who join in most on social and recreational activities?
Figure 2 Examples of Research Questions Asked in Fraser
house
In answering, patients
were not only being encouraged to notice healing micro-experiences (experience
of little bits of behavior that may contribute to healing), they were receiving
the strong positive emotional experience that what they thought and felt about
things mattered and was of value. Having come from conflicted family
environments where contradictory communication (Laing and Esterson 1964) was the norm, doing reality testing and checking the validity of
their observations was valuable. Patients and outpatients would start
discussing a very diverse range of topics and in the processes evolve their
capacities in forming, expressing and evaluating opinions.
Another example of
treating them with respect, dignity and worth was asking them to explore and
give answers to questions about their value systems. One of these questions was
almost a quote from Assagioli, that is, �The Spirit working upon and within all
creation is shaping it into order, harmony, and beauty uniting all beings�
VALUES
RESEARCH
Neville carried out extensive values
research based on the concepts of Florence Kluckhohn 1950 (Yeomans 1965). A list of
the questions that were asked in Neville�s Values Research is in Appendix 5. This
Fraser House values research was followed up by questionnaires being completed
by over 2,000 people in Sydney, Melbourne and Brisbane, the three largest
cities in Australia. A Survey called, �The Survey of the Youth of Victoria� was
conducted by the Good Neighbor Council and the Commonwealth Department of
Immigration Survey Section Canberra 1967. (Yeomans 1965, Vol 13) This survey collected information on
social and economic themes as well as attitudes and values. It used Neville
Values Questionnaire for the values component. There were 1035 informants and
1017 used in final analysis.
Substantially shifting core values amounts to shifting culture.
Chapter Nine discusses the Laceweb experience regarding the effect of changing
values, frames and behaviors at the level of everyday lived life, and the
potential of this in the longer term for producing social change; that was and
still is the potential of Fraser House/Laceweb healing energy. Neville stated
that at the time, this values research was, in all probability, the most
extensive research on values that had been done anywhere (Clark and Yeomans 1969, p. 20-26).
What
Do You Think About Trade With Asia?
Patients knew that all
manner of data was being collected about them relating to demographic and
socio-economic data, length of stay, participation by their friends and
relatives and the like. Research outcomes were discussed with patients. All
this research had parallels to patients being asked to be on committees. It had
the effect of involving them in participatory and humane democracy.
Participatory and humane democracy is discussed further in Chapter Nine in
relation to post-conflict situations like East Timor and Bougainville. This is
resonant with Neville�s later studies in humanitarian law and having humane law
and community democracy as foci in the Laceweb
(refer Chapters Nine and Ten).
Within a connexity based Cultural Keyline frame
it made absolute sense to ask psychiatric patients and ex-prisoners their
attitudes towards overseas trade with SE Asia, or about landscape planning and
urban renewal, or their thoughts and attitudes about crime and substance abuse.
This is consistent with the Hawthorne effect. It engaged them as people of
worth and encouraged them to see their place in their local place linked to the
Region.
Neville told me that a process he
used to protect Fraser House was that a number of research workers from Sydney
Universities carried out research at Fraser House obtaining higher degrees. To
close Fraser House would have meant closing many students research. Alfred
Clark had his PhD on Fraser House under way. Margaret Cockett was doing her
Masters research in Anthropology when the keeper of Unit�s records discarded
all of her material and they were burnt, therefore aborting that degree (Yeomans
1965, Vol.12, p.68).
Margaret suspects this destruction was deliberate, because of a sustained and
pervasive dislike of Fraser house by elements within the wider North Ryde
Hospital. Margaret later obtained her masters based on different research. I
have found no records of Fraser House in Health Department Records. It is as if
it never existed.
Margaret Cockett, also did
a lot of research making sociograms of networks within Fraser House using the
concepts of �power�, �opinion leaders�, �leaders� and �influence�. This was
brought to my attention by Warwick Bruen in a conversation I had with him in
August 1999. The doing of this research was later confirmed by Margaret
Cockett. Regrettably, this research was among the materials discarded by North
Ryde Hospital � perhaps an example of hostile attitudes held by some against
what was happening in the Unit. Like all of the other research, the results
were discussed with staff and patients, within groups and the progress
committee.
Appendix 6 and Appendix 7 lists
inventories developed and used at Fraser House (Yeomans 1965, Vol. 4 , p. 43) (Yeomans 1965, Vol. 11). These
inventories enabled the putting together of a holistic psycho-social emotional
mindbody portrait of each patient and outpatient�s whole life, covering
presenting matters, recent past, post-school period, childhood as well as work
history and recreational activity. This is consistent with the holistic
socio-emotional focus of change at Fraser House.
Despite being extremely
busy with every aspect of Fraser House and its links into the community,
Neville was very active in research and writing up papers. He was an active
presenter at conferences and other professional meetings. Appendix 8 contains
three Tables (A, B, and C) listing fifty seven of the extensive body of
Neville�s research papers and monographs mentioned in his collected papers in the
Mitchell Library. Many are undated though come from the 1959-1965 period.
Group and crowd behavior
during big groups was a constant research theme. For example, Neville used the terms �Collindivism�
and �Colindivity� to described the nature of interaction at Fraser House (Yeomans 1965). The terms (col from
collectivities and indivity from individuals) referred to a gathering of
individuals and collectivities interacting as individuals and collectivities.
The most frequent collindivities would
be those including both the extreme individualists and extreme collectivists
working together on a common problem in interaction. The collectivists would
tend to function as parts of a team and for its stability, while the
individualists would function as single entities and for their own separate
stabilities. Such a subgroup of individualists could be called an indivity',
that is, a collectivity functioning under an individualistic ideology with its
individual units primarily fostering the reality of their own systems; for
example, �an international gathering of extreme nationalists� (reference).
Neville fostered a climate that supported indivity and collindivity. Fraser House became a center for studying Group and crowd
behavior. This is discussed later.
Fraser House research
served at least two other functions. Results were fed back in to modify the
structure, process and action research in the Unit. For example, the critical
and destructive role of extremely dysfunctional families and friends in holding
back patient improvement became clearer to staff and patients alike from both
experience and research over the first three years. Greater efforts were then
made to involve these networks.
The research was used to
protect the Unit and ensure its survival, at least for a time. Research
outcomes and the evaluation of Fraser House are discussed later. Neville set up
the Psychiatric Research Study Group as an integral aspect of Fraser House
Research. This is discussed in the following section.
PSYCHIATRIC
RESEARCH STUDY GROUP
During the early days of
Fraser House and as part of Neville�s passion for inquiry and continuous action
research on networking, he formed the Psychiatric Research Study Group. This
was an early example of Neville enabling networking and learning about
fostering self-organizing emergence. Neville set up the Psychiatric Research
Study Group on the grounds of the North Ryde Hospital adjacent the Unit. The
Group was a forum for the discussion and exploration of innovative healing
ideas. The study group networked for, and attracted very talented people.
Students of psychiatry, medicine, psychology, sociology, social work,
criminology and education attended from the University of NSW and University of
Sydney and other places. The Psychiatric Research Study Group became a vibrant
therapeutic community in its own right with a connexity relation with Fraser
House. Prison officers and parole officers with whom Neville had been working
within the prison and corrective system attended the Study Group. Tony Vinson
also attended the study group. He is now Emeritus Professor at the School of
Social Work at the University of New South Wales. Neville spoke of Tony Vinson
doing sociology studies in the early Sixties, obtaining his PhD in 1972 and becoming
the Foundation Professor of Behavioral Science in Medicine at the University of
Newcastle in 1976, and Chairman, of the NSW Corrective Services Commission in
1979. A 1963-65 Research Report states that, �Tony Vinson and his team of
Social Work 11 students from the University of NSW, with the Fraser House
research Team, for a time acting in an advisory capacity regarding research
design and field work methods, carried out a study to assess the effectiveness
of the Lane Cove Community Aid Service and the Fraser House Community
Psychiatric Programme� (Yeomans
1965, Vol. 12, p. 45-90).
Students and others would
present papers at the Psychiatric Research Study Group and passionate discussion
would follow. Many of the attendees could not, or would not discuss their ideas
within their respective university departments. In the University environment
of the day, some were scared of presenting certain of their papers because of
their innovative and groundbreaking content. Some had tried and could not get
an audience for their ideas.
The Study Group provided a space where
ideas that would in all probability have been rejected out-of-hand in other
forums, were enthusiastically received and discussed. The Study Group was
another cultural locality. Anything raised in the Study Group that seemed to
fit the milieu in Fraser House was immediately trialed by Neville in the Fraser
House. In trying something to see if it worked Neville spoke of �the survival
of the fitting�. Margaret Mead chaired the Psychiatric Research Study Group
when she visited Fraser House as head of the World Mental Health Federation (Yeomans 1965, Vol. 12, p. 68).
At one time there were 180 members on
the Psychiatric Research Study Group mailing list. Neville wrote that the Study
Group, �Represents every field of the social and behavioral sciences and is the
most significant research institute in this State.� �The Psychiatric Research
Study Group maintained a central file of research projects underway throughout
NSW and acts in an advisory and critical capacity to anyone planning a research
project� (Yeomans 1965, Vol. 4 , p. 24). Meetings were held monthly at first at
Fraser House and then elsewhere. Margaret Cockett said that during the 1970�s
she was continually meeting up with all manner of very interesting people who
had links to Fraser House and the Psychiatric Research Study Group.
WORK
AS THERAPY
As stated above, the
canteen provided one context for using work as therapy. Another example was the
patients winning a contract to build a bowling green against �outside�
contractors. This involved the tendering, winning and carrying out of a
construction/landscaping contract to build a bowling green for Fraser House.
The patients controlled every aspect of the tendering and work.
Photo 5 Patients building the Fraser
House bowling green in the Sixties.
Photo from Sydney Morning Herald
Clipping in Mitchell Library
The above photo above was
taken in August 1999. It shows the Bowling Green area behind the fence that was
leveled out by patients with hand tools. The retaining wall was also built by the
patients and it has stood the test of time - still vertical
This was the therapeutic use of an
actual economy, not token work as used in United States Research by Paul and
Lentz (Paul and Lentz 1977). The link between this US research
and Fraser House is discussed in Chapter Seven.�
A very important type of
work that some of the patients became very adept at was being therapists and
co-therapists in group contexts. Often the most insightful therapy in everyday
life within the community was by patients. Their therapy work extended to Big
Group, the small groups, interrupting incidents within Fraser House, support to
specialed patients (discussed previously), individual therapy, everyday life
context therapy, getting the agreement of friends, workmates and relatives to
attend Fraser House Groups, domiciliary care to ex-patients and outpatients,
the on-call community suicide and crisis support service and therapy skills
training for new staff and guests including training of psychiatrists learning
the community psychiatry component of their psychiatric course. Fraser House
became the main center for training in community psychiatry.

Photo 6 Photo taken in 2000 showing brick retaining wall
and bowling
green behind wire-mesh fence
MEDIATION
THERAPY
Neville refined a form of therapy where �mediation� was a
descriptor (adjective) of the process. Many
years later Renouf (Renouf 1992)
wrote of the uneasy sixth step in mediating - that of a form of mediating that
is inherently building and healing relationship. Almost invariably,
conventional mediators are not equipped
to engage in this type of process and do not attempt to do so. Neville�s
mediation-therapy requires a fundamentally different set of healing and
therapeutic processes and competencies/abilities compared to those typically
used for mainstream mediation.
Neville placed me in sustained action research contexts using
mediation therapy to refine my competencies. Chapter Eight discusses Neville�s
pioneering contribution in the use of mediation within the Family Law process,
and within law, neighborhood disputes, and the business community.
A
FOLLOW-UP SERVICE AND LIAISON WITH OUTSIDE ORGANIZATIONS.
Fraser House offered primary patient
care by skilled psychiatric nurses to many surrounding organizations. A Fraser
House social worker was based in the Hunters Hill Council Chamber�s
Administrative Office providing a service to the public half a day a week.
Neville was continually giving talks to church groups and other organizations
about Fraser House and it�s processes. Neville set up what was called the
Sydney Therapeutic Club on verandah of Ward One at Sydney Hospital (Yeomans 1965, Vol 5, p. 104). Neville worked closely with eight
social workers at Sydney Hospital. Some of the social workers were trained in
group therapy and a consultative mental health programme was established. Six
of the social workers attended Fraser House groups. Sociotherapy groups were
held regularly at Sydney Hospital for three years (Yeomans 1965, Vol 12, p. 70). Fraser House patients and
ex-patients attended these Sydney Hospital Groups. Neville announced the start
of these Sydney Hospital sociotherapy group meetings during a Fraser House Big
Group that was very tense, as a catalyst for change in that Big Group�s mood
(refer �stimmung� mentioned previously).��
As an example of linking Fraser House to the
wider community and vice versa, during 1965 assistance was given on an
individual or workshop basis by members of the Fraser House Research Group to
thirteen organizations listed in Appendix 9 (Yeomans 1965, Vol.
12, p. 94). Seventeen people
from the Parramatta Psychiatric Center met monthly under Neville�s chairmanship
on eight occasions. (Yeomans 1965, Vol.
12, p.85) Members of the
Salvation Army undertook training in group leadership at Fraser House. Brief
and extended training courses also included clergymen from all Christian
denominations. Also involved were family welfare agency counselors, parole
officers and nurses and administrators from private hospitals. Neville also
advised the Salvation Army on the development of hostels (Yeomans 1965, Vol,
12, p. 72). Neville was the Honorary Consulting Psychiatrist at Langton
Clinic for Alcoholics. He also guided that hospital on therapy, policy and
research (Yeomans
1965, Vol. 12, p.70)
��������������������������������������������������������������������������������������������������������������������������������������
����������������������������������������������������������������������������������������������������������������Neville
also gave many talks and interviews about Fraser House that were broadcast on
TV and radio. This was confirmed by Neville, Chilmaid, and Bruen. Neville was
the Guest of Honor at the All Nations Club on 30 August 1963 (All Nations Club 1963). A draft of speech on social problems
to the Ionian Club Sydney entitled �Introduction on the Origins of the Ionians�
is included in Neville�s archived papers (Yeomans 1968, Vol. 1 p. 291. ). On one occasion a TV crew from the
ABC came and filmed a section of Big Group. One of the intentions of these
interviews was to have the public know so much about what was happening at
Fraser House, that it would raise a hue and cry if there were any moves to
close the Unit.
Neville was away overseas for nine months in 1963 exploring the
state of the art in community based healing approaches in the United States and
the United Kingdom. In Neville�s view Afro-American community child care
centers and community welfare centers were �state of art�; they were looking
after their own. Upon his return Neville wrote a report recommending that
community mental health centers be attached to schools, because school
counselors meet the families. Neville�s report recommendations were shelved.
Neville energized the Paddington Children�s� Community Center based in part on
the Afro-American New Haven Community School he visiting in America (Yeomans
1965, Vol. 1, p70-80).
This linking of support to schools has some resonance with what happened in the
NSW town of Bourke as a result of two Aboriginal members of that Community
attending a Human Relations Gathering enabled by Neville in Armidale, NSW in
1971. This is discussed in Chapter Eight.
FRASER
HOUSE TRAINING
Such was Fraser House�s growing reputation in the new field of
�community psychiatry� that Fraser House became the place providing community
mental health training in community psychiatry for students preparing to become
members of the Royal Australian and New Zealand College of Psychiatry. Students
were allocated to Fraser House for six-month periods. Social worker students
from both the University of Sydney and the University of NSW were also trained �(Yeomans 1965, Vol. 12, p.73). Dr William (Bill) McLeod, head of Royal Park Psychiatric Center
in Parkville, Victoria for many years told me in 2002 that in the early
Eighties he used Neville as an examiner for the Royal Australian and New Zealand
College of Psychiatry.
Neville and Margaret
Cockett both confirmed that they and Harry Oxley prepared a course introducing
psychiatrists and also medical students to the sociology of medicine,
socio-medicine and anthropology. They then began lecturing in this course
through Callan House. This was the first course of this type. I have
been unable to track down any records of this course.
CATCHMENT
AREAS
Fraser House was the first
mental institution in Australia to identify surrounding suburbs as an area of
�special interest�. Church and other community groups in the area were
approached and told about the programs and processes used at Fraser House.
Neville was a frequent speaker at these groups. People from the groups were
invited to attend Fraser House as guests at Big and Small Groups. Fraser House
research people gathered data relating to the mental health in the surrounding
area. This area came to be known as Fraser House�s �catchment area� (Yeomans 1965, Vol 4. p. 2-4).� Neville
supported the setting up by Dr Mitchell of a therapeutic community in the very
large Kenmore Hospital in Goulburn. They were one of the first to follow Fraser
House in using catchment areas (Mitchell 1964). The Kenmore Therapeutic Community is discussed in Chapter Seven.
This notion of catchment areas has spread through mental health services. This
was an innovation that contributed to the demise of Fraser House as total and
voluntary therapeutic community. In 1968, the areas around Lane Cove were
designated the �Admissions Catchment Area� for Fraser House, and from then on involuntary
patients (people being committed) were admitted to Fraser House. This
fundamentally distorted and collapsed the Fraser House voluntary self-help
process.
MARGARET
MEAD VISITS FRASER HOUSE
The Anthropologist
Margaret Mead visited Fraser House as the Co-Founder (1948) and ex-President (1956/7)
of the World Federation for Mental Health (Brody; 2002). Margaret Cockett informed me that Margaret Mead was introduced
to Fraser House by an anthropologist friend of Margaret Cockett in the Housing
Department who had told Mead about Fraser House when she came to visit her.
Margaret Cockett told me that initially Margaret Mead could not believe what
she was hearing and came to Fraser House to check it out. Mead was escorted throughout
the day by Margaret Cockett, the Fraser House anthropologist psychologist. In
an interview I had with Margaret Cockett (Aug 1999) she recalled Margaret Mead
saying that she was very taken with the concept of therapeutic community and
had visited many such communities in different places. Mead also stated that
Fraser House was the only therapeutic
community that was totally a
therapeutic community in every sense.
In talking about her feel for Fraser House�s totality and completeness Cockett
said that Mead spoke of Fraser House as the most Total therapeutic community she had ever been to. Mead was
particularly taken with the fact that important others were required to
regularly visit patients in Fraser House, and that one patient, having a horse
as the only �important other� in her life, was allowed to have the horse
tethered grazing on the lawns of the hospital just outside Fraser House. A few
other patients had a cat or a dog as their �important other�.

Photo 7 These Are the Grounds Outside Fraser House Where
the Horse Grazed
In August, 1999 interview
Chilmaid said that the �total� nature of the therapeutic community was a major
factor in limiting violence as well as suicide. Mead very ably conducted the
morning Big Group as well as small groups.�
Margaret Cockett described Mead as being �absolutely on the ball� in the
role of leader of both Big Group and one of the small groups. Margaret Mead
also took the regular half hour staff group meeting that followed the Big
Group.
Many �big men� from the
health department joined Margaret Mead for lunch where according to Margaret
Cockett, Margaret Mead held court and demonstrated that she was clearly ahead of
every one of them in their respective specialist areas. Margaret Cockett
suspects that it was Margaret Mead�s glowing report to these people in the NSW
health establishment hierarchy that made things just a little easier for Fraser
House for a while. At that time, the medical and psychiatric profession saw no
relevance whatsoever for anthropology in their professions. Margaret Mead gave
the �big thumbs up� to Fraser House to these Department Heads, �heaping praise�
on every aspect of the Fraser House therapeutic community. Neville had
completed a file note on this visit by Mead (Yeomans 1965, Vol. 12,
p.69). The file note says �Dr.
Margaret Mead, world famous anthropologist who visited Australia last year
attended a meeting of the Psychiatric Research Study Group and also stated that
she considered Fraser House the most advanced unit she had visited anywhere in
the world.�
CASE
HISTORIES SHOWING GLIMPSES OF THE FRASER HOUSE MODEL IN ACTION
The
Nurturing Mother
A mother was serving
twelve years for the murder of two of her three very young children. Right
through the mother�s prison term she had repeatedly stated that she was waiting
for the day she gets out of jail to kill the remaining child. This child had
been looked after by foster parents for eleven years and was twelve years of
age. When the mother was within a few months of release she was still
threatening to kill the child. There was a lot of pressure from the prison
authorities on the Parliament of the day to pass special legislation to ensure
this woman was never released. Prison governors and warders alike were
concerned for the safety of this remaining child. Upon learning of the fears
about the mother and her pending release, Neville suggested to the authorities
that the mother be allowed to request a transfer from prison to attend Fraser
House on a voluntary basis and if she agreed, to grant her request. In process
of setting up this possibility, the foster parents of the surviving child,
along with the child in question were invited by Neville to attend Fraser House
Big and Small Group meetings for a number of months while the mother was still
in prison. Neville fully briefed the foster parents and child on Big and Small
Group process so that they all knew what to expect. The Foster parents and the
child agreed to attend. There were other children present, as was the custom -
up to eight families were in residence at any one time. As well, families and
friends visitors included children. The safety of children and everyone was always of paramount
concern. As for high expressed emotion and children, typically, in these
families children already had been living with it from birth.
This
attending of Big Group was for the foster parents and the child to firstly,
decide whether to be present in Big Group if and when the mother arrived, and
secondly, so that they could all get a sense of how Fraser House �operated� on
dysfunctionality, and thirdly, so that they could potentially - if the mother
was released into Fraser House - have some clarity about where the mother was
at. The alternative was for the child and foster parents to live, knowing the
mother was possibly to be released, and then at large, �somewhere out there�,
and knowing she was still threatening to kill the child. After regular
attendance at Big and Small Groups, the foster parents and the daughter agreed
to be present if and when the mother arrived at Fraser House. Given the
circumstances, this says a something about Fraser House.
Also saying something
about Fraser House and the spirit of the times, it was agreed by the
Authorities that the mother be given an ultimatum - �be escorted from prison
directly to Fraser House and admit yourself voluntarily or we will pass
legislation to keep you in prison indefinitely�. She accepted the Fraser House
alternative. The foster parents and child agreed to leave it up to Neville
whether or not to introduce them to the mother, and when. That the child and
Foster parents were attending Fraser House groups, wanted the mother at Fraser
House, and that the three of them would be there when the mother arrived was
made known to the various interested parties determining the mother�s release.
However, the maternal mother was given no information of the intention to have
her daughter and the foster parents present on the day she arrived. When the
mother was ushered into Fraser House she had little idea where she was or what
sort of place Fraser House was - all she knew was that it was a psychiatric
hospital where she would have a better chance of release compared to staying in
prison where she was facing the possibility of an indefinite prison term. The
members of the small assessment group who interviewed the mother upon her
arrival were all patients who had killed or seriously injured members of their
own families - it takes one to know one.
This assessment was by
members of the Admitting Committee made up of patients and was a regular
feature of Fraser House. They did not declare they were patients and that they
had all murdered or had seriously injured their family members.
The maternal mother had
had no information at all about her sole surviving daughter for the eleven
years she had been in jail. She had no knowledge of her daughter�s current
whereabouts and that she would potentially meet her daughter in a Big Group
setting. The maternal mother was left in the care of a staff member while the
assessment group briefly gave their initial assessment of her state to the
waiting Big Group. The mother was then taken down the short (soundproof)
passageway and into this rather small room crammed to capacity. Around 180
people were in two tight circles and all eyes were on the mother. She was
totally unprepared for this. She searched the room for familiar faces and found
the members of the Assessment Group. She was directed to a spare chair and
hardly noticed that she was sitting between two very powerfully built men. With
their casual clothes, she had no way of knowing they were nurses who had been
placed either side of her to prevent her reaching and harming her daughter.
Beside one of the men was a female nurse. Unknown to the mother these three
were on constant alert to stop her approaching her daughter. Directly opposite
sat her daughter flanked by her foster parents who in turn were flanked by
people also on constant preparedness to move together and forward to block the
mother being able to reach the daughter.
Neville spoke up and asked
members of the Assessment Group in turn to give the newcomer their backgrounds.
Each spoke briefly of assaulting/killing members of their families. After the
overwhelming confusion and emotional flooding from this introduction to Fraser
House Big Group, Neville caught the mother�s attention and said words rather
quickly and matter of factly to the effect, �and....by the way....over there is
your daughter... mentioning her name.�
Already in overload from
the weird context, this sudden potent unexpected revelation put the mother into
massive overload. The mother now had the opportunity to have a shot at killing
her daughter in front of the group. This had been her fantasy obsession for
eleven years and here was her daughter in the flesh in front of her - just a
few steps away! After a very short time in the room the mother suddenly made a
frenzied dash towards the girl and the male nurses, on razor alert for just
such an occurrence, grabbed the mother. She immediately went into an almighty
struggle with super-human emotional energy. The female nurse grabbed the
mother�s hair and pulled this to restrain the mother from her attempts at
biting bits off the two male nurses heads and shoulders. There were others
prepared on either side of the foster parents and child (in the middle) that
headed towards the mother blocking her path to the foster family. When she was
restrained the meeting resumed. After a time when she had calmed a little, the
restraining hands left her. She made a couple of other dashes and the same
process returned her to her chair. The mother, daughter and foster parents were
the group focus for the balance of the hour. The mother was probed relentlessly
to determine where she was at.
Nothing, absolutely
nothing, altered Fraser House routines. The Big Group meeting always lasted
sixty minutes - exactly. The four key people in this case, sometimes
separately, sometimes in different combinations attended the regular and
special small groups that occurred throughout the day. They were again the
focus of these groups. The maternal mother was not left alone with the
daughter. All four participated in the evening Big Group. It emerged that at
the time of committing the offences until she arrived in Big Group, the mother
had had a delusional belief that all her children had a disease that would
blind them. This delusional belief was unraveled and dispensed with. After
everything that had happened that day, at the end of the evening Big, Small and
special Group meetings there was consensus among everyone present, including
the daughter and her foster parents, that the mother was now �safe�. She had had
an absolutely sustained nourishing and corrective emotional experience
throughout the day. Neville had plotted and planned for Fraser House to be at
it�s healing best. The whole community had been in large part focused on this
challenge for weeks.
The maternal mother and
the daughter stayed together alone in a bedroom that night!
The following day a staff
member wanted to know who the wonderful new nurturer was, and where was the new
�murderess�. It was pointed out that the �nurturer� and the �murderess� was
�one and the same person�. Neville describes having an overwhelming love for
this mother during the whole hour of Big Group, during the balance of the day
and thereafter.
The
North Shore Bus Depot Gang
One prisoner who was to become
the leader of the North Shore Bus Depot Gang was described as an incorrigible
con man by all who knew him. He pretended to be schizophrenic and specifically
requested a transfer to Fraser House from Long Bay Prison in Sydney. The
correction authorities/parole people were open to this shift and on hearing of
the request, Neville accepted him, recognizing that he was in no way
schizophrenic. When things were not going as easy as planned by this
ex-prisoner, he demanded that Neville send him back to Long Bay. Neville
instantly agreed and the con man instantly withdrew his request.
There was a culture of
disclosure in Fraser House - bring it up in the Big Group for the benefit of
everyone. Compassion was shown and ruthless people were kindly entrapped. Criminality
was undermined and subverted. This Long Bay Prisoner had formed a gang within
the Unit from within the �criminal element� of Fraser House patients. They had
realized that Fraser House was the perfect �criminal hide-out�. They were
planning to rob a major North Shore bus depot on the day the depot had a large
amount of cash.� A couple of fellows
started to have a change of heart and sensed that if the robbery happened it
could reflect badly on the Fraser House community. It could have Fraser House
closed!�
They confessed to a couple
of nurses who were taken to the place under the Fraser House building at the
back of the Eastern end where imitation guns and masks were hidden. The matter
was brought up at Big Group and the whole group was chastened. No vendetta took
place by the gang against informers as there was a constraining network of
factors to ensure this. Firstly, any small group contemplating payback would
have the total community against them. Secondly, some gang members were on
parole from prison and could be easily sent back there. They certainly did not
want this. As well, there was the reformative pressure of the total community
therapy process. Heightened crowd tension at Big Group was always used for
therapeutic purposes. In this case, �the threat to the community� was a major
component of the change potency of that Big Group. In addition, there were
standing arrangements for police to have a quiet talk with clients if
necessary. The gang members knew there would be no hesitation in doing this as
it had happened a number of times. For example, on a tip-off from Fraser House,
police would call around to the homes of absconders, especially those with drug
habits and thieving records and tell them to get back to Fraser House or there
would be trouble. Typically these absconders would turn up back at Fraser House
looking rather sheepish. Neville has no recall of police ever coming into
Fraser House. The police did however go under Fraser House to retrieve a person
wanted by the police who was being sustained by some patients.
I
had occasion to meet this ringleader of the �North Shore Bus Depot Gang� in the
early nineties around 25 years after his release from Fraser House. With
Neville, I was visiting Petford Aboriginal Training Farm, a remote Aboriginal
Therapeutic Community. The former �gang leader� was at the same community doing
some criminology research for a former criminologist with the Australian
Institute of Criminology in Canberra.� It
was after some hours of three-way discussion that Neville invited the �gang
leader� to chat about how he had first met Neville. That�s when he revealed his
former life as �bank robber�. I would never have picked him! The ex-gang leader
made it very clear that after his involvement with the Fraser House experience
he was, to use his words, �a completely different person�. He talked about the
Australian Institute of Criminology and how he became a personal
assistant/field researcher there, a role he had for a number of years.

Photo 8 The Rear of the Building Where the Gang Hid Their
Gear.
REFLECTING
ON FRASER HOUSE �TREATMENT� APPROACHES
Every aspect of the design
and redesign of the Yeomans action on their farms was pervasively integrated.
It was, to use Neville�s phrase again, the �survival of the fitting�. Neville
and his father knew that it was virtually impossible to control a living
system. Living systems have self-organization as an inherent property. Neville
and his father keenly attended to how the natural systems �worked� on the farm
and designed their interventions to maximally fit with nature and allow
nature�s emergent properties to do what they do so well. Neville took this
model across to Fraser House. In mirroring Indigenous way Fraser House was
about fostering respectful co-existence and meaningfully surviving well
together. Everything he did in Fraser House was designed to fit with everything
else - naturally. Everything complemented and supported other aspects. Things
that did not work were fine tuned or discarded. Issues that arose in one
context were resolved or passed on to other contexts. What worked as well as
problematic aspects were discussed with everyone in Big Group. Issues not
resolved in Big Group were passed on to Small Groups and vice versa. Issues within
Committees were resolved, or passed on to Parliamentary Committee. Issues
within the Parliamentary Committee were reviewed by the Pilot Committee. This
is why Margaret Mead said it was the most
complete therapeutic community she had ever seen and why Maxwell Jones said
that participants in Fraser House had
to change.
To use Keyline metaphors,
in Fraser House Neville was breaking new ground with cutting edge
processes turning the eroding rush of dysfunctional life, and enabling
people to self organize in obtaining a right angle on things for heading
in gentler and more thrival directions for fertile
possibilities to emerge. In this, many of the words traditionally used in
mental asylums were hardly appropriate � words like, �therapy�, �treat�,
�treatment� and �heal�. Each of these has surplus meaning associated with the
notion that �experts make unilateral decisions about doing things to another
person that will �fix� them�. In Fraser House they still used words like the
above four, though understood them in terms of the Unit�s milieu.
Perhaps new words need to
be evolved that encapsulate the concepts explored in this research. For
example, the word �treatment was in the previous paragraph. Neville was not
into a process whereby people were �treated� (as in �we will fix you�) by
professional experts. Intervention by professional experts was expressly
structured out of the process.
Neville�s approach and that of all of the Fraser House community was
�generalist� rather than �diagnostic�. Neville had no difficulty with diagnosis
per se. He was a member of the Committee of Classification of Psychiatric
Patterns of the National Health and Medical Research Council of Australia.
Fraser House was not a place of �service� delivery in the conventional sense.
If anything, the people involved were treated, as in �given treats� at times of
partying and celebration. They were �treated� in this sense by giving them the
gifts of joy, care, love, respect, compassion, and the company of tough,
caring, loving, community associates who just would not let them persist in
being crazy. The Staff did �serve� in the sense of �enabling support�, though
this in no way a �service� in the normal sense. There are major differences
between �service delivery� and self-help. Neville, Terry Widders, an Aboriginal
colleague who Neville worked closely with, and myself had an occasion to write
a monograph on the difference between �service� and �self-help� that was sent
to an Australian Federal Government Health Department. The paper was entitled,
�Government and the Facilitating of Grassroots Action� (Yeomans, Widders et al.
1993; Yeomans, Widders et al. 1993). This will be discussed later. Everything points to Fraser House
patients and outpatients �treatment� resulting in major normalizing changes
occurring in their manifest mad/bad �symptoms� and functional responding in the
World (Madew, Singer et al.
1966; Yeomans 1980; Yeomans 1980). Coincidently, the co-author in the previous reference,
psychologist Professor Peter Singer, moved to the psychology Department at La
Trobe University where he was one of my lecturers.
Neville was familiar with the
reciprocal concepts, �Society is a socially constituted reality� and
simultaneously, �Society produces people as social products� discussed by
Berger and Luckmann and told me that this was particularly germane to Fraser
House process where people were reconstituted as they jointly co-reconstituting
the Fraser House shared reality (Berger and Luckmann 1967). The shared life in the close community meant that helping and
supporting each other was structured in. Treatment was based on the notion that
emotional corrective experience was
central to transforming to being well. The record of patient return to
community and functional living, along with recidivism rates was significantly
better than mainstream hospitals, and was effected at a significant lower cost (Yeomans 1980; Yeomans
1980).
A
MODEL FOR THE WORLD
Fraser House became a model for the World and
a powerful influence in closing mental asylums. No asylums have since been
built in Australia. Central to Neville�s Cultural Keyline Way was enabling
living systems so that aspects, and especially latent emergent properties of
the system, self organize into a
better thriving. At Fraser House the challenge was how to set up natural
structures and processes that were isomorphic (of matching form) to what
Neville and his father had work so well for them naturally in their Keyline
work. In the farm living system context, the key elements were warmth, air,
water, soil biota, and dead organic material.
In Fraser House the key
elements in the situated living system were the free energy (potential for
thriving) within mad and bad people and their family/friendship networks, the
interactive potential of situated psychosocial-emotion within internal spaces
and places (as in Tikopia - (Firth 1957)) of the Fraser House cultural locality, and within the various
localities and places/spaces patients and outpatients would be returning to,
and the enabling resources and commitment of staff. Into all of this Neville
wove Indigenous socio-medicine for social cohesion (Cawte 1974; Cawte 2001,
(First edition - 1996)).
This Chapter has begun the
exploring of Neville�s adaptation of Keyline to the psychosocial sphere. It
described how Neville used his Way to enable all involved in Fraser House, as
community, to devise and revise their own
structures and processes. Big Group and Small Groups based on Sociological
category and other innovative change processes including Big Group, Small Groups
and other processes used by patients and outpatients (and staff) to transform
their lives towards living well have been specified.
Chapters Six and Seven provide a
synthesis relating to Neville�s evolving and use of Cultural Keyline within
Fraser House in linking the psychosocial with the psychobiological.
Criticisms about Fraser
House and Neville are outlined and responded to. The processes Neville used to
spread Fraser House Way into the wider community and phase out Fraser House are
described. The Chapter concludes with a brief discussion of ethical issues in
replicating Fraser House.
(1960).
Alcoholics v Neurotics - They Fight it Out at the Clinic. Sunday Telegraph.
Sydney.
(1960). Love From a Stranger. Readers
Digest.
(1960). Pulled From Brink - Suicide
Clinic. The Sun. Sydney.
(1960). Suicide Urge - Clinic Saves
Lives: Fraser House - The Neurotic and Alcohol Unit of the New Psychiatric
Centre at North Ryde. The Sun. Sydney.
(1961). Are you a Potential Suicide? Pix: p. 14-15.
(1962). Why Do People Commit Suicide? Sunday
Telegraph. Sydney.
(2002). World Federation for Mental
Health� Homepage - Internet Source - http://www.wfmh.org.
Alexander, F. (1961). The Impact of
Freudian Psychiatry. [Unive#].
All Nations Club (1963). Invitation to
Hear Dr Neville T. Yeomans Speak at the Next Meeting as Guest of Honour.
Sydney.
Bandler, R., J. Grinder, et al.
(1982). Reframing : Neuro-linguistic Programming and the Transformation of Meaning.
Moab, Utah, Real People Press.
Berger, P. L. and T. Luckmann (1967). The
Social Construction of Reality : A Treatise on the Sociology of Knowledge.
Garden City, N.Y., Doubleday.
Bootes, B. (1978). Lifeline
(Melbourne): A Case Study on Training People to Run Lifeline. :. Bundoora,
Preston Institute of Technology Publishing.
Brody, E. B. The Search for Mental
Health - A History and Memoir of WFMH 1948-1997.
Castaneda, C. (1974). Journey to
Ixtlan. Harmondsworth, Middlesex, Penguin Books Ltd.
Cawte, A. (1974). Medicine is the
Law - Studies in Psychiatric Anthropology of Australian Tribal Societies.
Adelaide, Rigby.
Cawte, J. (2001, (First edition -
1996)). Healers of Arnhem Land. Marleston, SA, J.B. Books.
Clark, A. W. and N. T. Yeomans (1969).
Fraser House - Theory, Practice and Evaluation of a Therapeutic Community.
New York, Springer Pub Co.
Cockett, M. and P. Chilmaid (1965).
Significant 'Break-Throughs' Following Major Crisis. Fraser House
Unpublished Staff Research. Sydney.
Dean, S. R. (1971). "The Role of
Self-conducted Group Therapy in Psycho-rehabilitation: A Look at Recovery,
Inc." American Journal of Psychiatry 127(7): 934-937.
Dilts, R., J. Grinder, et al. (1980). Neuro-Linguistic
Programming - Volume One - The Study of the Structure of Subjective Experience.
Cupertino, California, Meta�
Publications.
Firth, R. (1957). We, the Tikopia :
a sociological study of kinship in primitive Polynesia. London, Allen and
Unwin.
Goffman, E. (1974). Frame analysis
: an essay on the organization of experience. Cambridge,Mass, Harvard
University Press.
Green, A. (1959). Dial SUI to Save
Your Life. Weekender. Sydney.
Hanlon, W. D. (1987). Taproots:
Underlying Principles of Milton Erickson's Therapy and Hypnosis. London,
W.W. Norton & Co.
Kelly, V. (1962). 880281 - A Phone
Number Saves 20 Desperate Lives a Week at the Suicide Clinic. The Sun.
Sydney.
Laceweb-Homepage (2001). Second SE
Asia Oceania Australasia Trauma Survivors Support Network Healing Sharing
Gatherings - July 2001 - http://www.laceweb.org.au/indexA.htm.
Laing, R. D. and A. Esterson (1964). Sanity
Madness and the Family. Harmondsworth, Middlesex, Penguin Books Ltd.
Lankton, S. R. (1980). Practical Magic
: A Translation of Basic Neuro-Linguistic Programming into Clinical
Psychotherapy. Cupertino, California, Meta Publications.
Madew, L., G. Singer, et al. (1966).
"Treatment and Rehabilitation in the Therapeutic Community." The
Medical Journal of Australia 1:
p. 1112-14.
Mercer, J. (2000). "Welcome to
the Johnny Mercer Educational Archives - Internet Source - www.johnnymercer.com/lyrics.htm."
Misang, J. (1998). A Personal
Communication About the Way of the Rataiku People of Bougainville. N. Yeomans
and L. Spencer. Yungaburra, Qld.
Mitchell, D. N. M. (1964). The
Establishment and Structure of Kenmore Therapeutic Community. Goulburn,
Kenmore Hospital.
Paul, G. L. and R. J. Lentz (1977). Psychosocial
Treatment of Chronic Mental Patients - Milieu Versus Social-learning Programs.
Massachusetts, Harvard University Press.
Pelz, W. (1974). The Scope of
Understanding in Sociology : Towards a More Radical Reorientation in the Social
and Humanistic Sciences. London, Routledge & Kegan Paul.
Petford Working Group (2000). The
Healing Art of Storytelling - Internet Source - http://www.laceweb.org.au/sty.htm.
Renouf, A. (1992). "The Uneasy
Sixth Stage of Mediation." Australian Disputes Resolution Journal 3(4 November): 257.
Satir, V. (1972). Peoplemaking.
Palo Alto, Calif., Science and Behavior Books.
Satir, V. (1983). Conjoint family
therapy. Palo Alto, Calif, Science and Behavior Books.
Satir, V. (1988). The new peoplemaking.
Mountain View, Calif., Science and Behavior Books.
Satir, V. M. (1964). Conjoint
Family Therapy: A Guide to Therapy and Te#. [Scien#].
Trahair, R. C. S. (1984). The
Humanist Temper : The Life and Work of Elton Mayo. New Brunswick, N.J.,
U.S.A, Transaction Books.
von Sommers, T. (1960). Dial the
'Club' and Talk it Over - Men Who Stop Suicides. The Sun. Sydney.
Wijewickrama, D. (2001).
"Chiropractic and Cybernetics." Journal Of Chiropractic Humanities?(?).
Wolff, K. H. (1976). Surrender and
Catch -� Experience and Inquiry Today. Boston
Studies in the Philosophy of Science. R. S. Cohen and Wartofsky. Boston, D.
Reidel Publishing.
Yeomans, N., T. Widders, et al.
(1993). Governments and the Facilitating of Community Grassroots Wellbeing
Action - Internet Source - http://www.laceweb.org.au/gfg.htm.
Yeomans, N., T. Widders, et al.
(1993). Governments and the Facilitating of Community Grassroots Wellbeing
Action., Report sent to Rural Health Support, Education and Training - Federal
Health Department, Canberra.
Yeomans, N. T. (1965). Collected
Papers on Fraser House and Related Healing Gatherings and Festivals - Mitchell
Library Archives, State Library of New South Wales.
Yeomans, N. T. (1965). Eight Social Workers
at Sydney Hospital. Neville T. Yeomans Collected Papers 1965, Vol. 12, p.
70. Sydney.
Yeomans, N. T. (1965). A General
Theory of Welfare Functions. Neville T. Yeomans Collected Papers 1965, Vol.
2, p. 38 - 40. Sydney.
Yeomans, N. T. (1965). Sociotherapeutic
Attitudes to Institutions - Paper Presented at the State Psychiatric Services
Clinicians' Conference - 22 April 1963. Neville T. Yeomans Collected Papers
1965, Vol. 12, p. 46, 60-61. Sydney.
Yeomans, N. T. (1966). Collective
Therapy - Audience and Crowd - Australian Journal of Social Issues 2. 4. Neville
T. Yeomans Collected Papers 1965,Vol. 1, p,187-188, Vol.12, p. 77, 87.
Sydney.
Yeomans, N. T. (1968). Draft of Speech
on Social Problems to the Ionian Club Sydney - Introduction on the Origins of the
Ionians. Neville T. Yeomans Collected Papers 1965, Vol. 1 p. 291.
Sydney.
Yeomans, N. T. (1980). "From the
Outback." International Journal of Therapeutic Communities 1.(1).
Yeomans, N. T. (1980). From the Outback,
International Journal of Therapeutic Communities - Internet Source - http://www.laceweb.org.au/tcj.htm.
Yeomans, N. T. ( 1965). Honorary
Consulting Psychiatrist at Langton Clinic for Alcoholics. Neville T. Yeomans
Collected Papers 1965, Vol. 12, p. 70. Sydney.
Yeomans, N. T. and L. Spencer (1993).
Cultural Healing Action - Internet Source - http://www.laceweb.org.au/cha.htm.