Chapter
Nine – Fraser House Transitionary Processes
INTRODUCTION
This chapter looks at Fraser
House small group process and the many other change processes evolved at Fraser
House. Margaret Mead’s visit is discussed and Neville’s adaptation of Keyline
to Cultural Keyline is analysed.
SOCIAL CATEGORY
BASED SMALL GROUP THERAPY
Just like Big Group,
Small Groups were run like meetings. Typically, one staff person ran the Small
Group and another staff person was a process observer, on-sider and trainee.
Small Groups were mainly conducted by the nurses, with some groups being lead
by medical officers, the social worker, and the chaplain. The chaplain ran some
spiritual groups at Fraser House. The Fraser House Handbook specifies the nurse
therapist role in Small Groups (refer Appendices 7 & 8):
The role of the Small Group therapist and
observer has always been the province of the nurse in Fraser House, and
represents part of the rise in therapeutic status. Nurses have become
therapists in their own right.
The first essential
in taking a group is to see it as a meeting, and like all meetings, there is a
need for a chairman to conduct affairs and keep issues to the point.
The initial function
of the therapist is to see that the group functions as a group (Yeomans, N. 1965a, Vol. 4, p. 18).
The Handbook then
gives detailed specifying of group process. Sections of the Handbook on the
Nurses Roles and Big Group process are shown in Appendices 7 and 8.
Small groups were
held from 11 AM to 12 Noon after a half hour refreshment break following big
group. They were preceded by the staff discussion over morning tea. After
evening Big Group and a similar thirty-minute staff discussion period, Small
Groups were run from 8 PM to 9 PM. During the staff discussion, patients and
visitors had an informal morning tea together separate from the staff. All
groups and the refreshment break ran strictly to time. Another staff discussion
meeting took place after Small Groups to ensure all staff was well briefed on
unfolding contexts.
In an April 2003 email Phil
Chilmaid wrote:
There were several ways to
follow up progress and issues: inter-staff verbal exchange at shift change,
ward report books, patients’ progress notes, and at various times, small group
report books, and a large sheet of butchers paper ruled up with boxes for all
the weeks programs and events so staff could come in after a gap or next shift
and follow themes and developments.
Generally, nearly all the outpatients (typically,
friends, workmates and relatives of patients) attending Big Group stayed and
were allocated to the various Small Groups in both the morning and evening
sessions. It was expected that outpatients attend both Big and Small Groups.
There were ten or more concurrent Small Groups typically made up of between 8
to 12 people, or more per group.
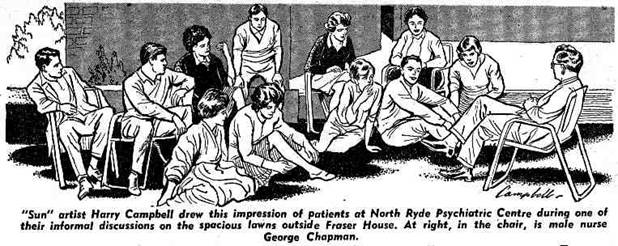
Drawing 1 A Sketch of a Fraser House
Small Group by Harry Campbell
The above illustration by "Sun" artist Harry
Campbell of patients at Fraser House was published in The Sun Newspaper, 17
July 1963, p.28 [Also included in Neville’s News clippings (Various Newspaper Journalists 1959-1974, p.
33-34)].
Recall that upon Tikopia there was constant linking
within and between people of differing generations, gender, clan, village,
locality, status (chief/non-chief families) and occupation, that is, between
differing sociological categories. Similarly, Neville cleaved Fraser House
family-friendship networks and inter-patient factions by sociological category.
Neville’s aim was to create self-organizing communal
living, which may impact upon and create shifts away from isolation and destructive
cleavage, or make functional cleavage in entangled pathological networks.
In
supporting mad and bad people with their dysfunctional family-friendship
networks live well with each other, Neville’s view was that one of the primary
healing processes that was both structured into and continually and pervasively
at work within Fraser House, was the day-to-day lived-life dynamic healing
interplay of social cleaving and unifying processes – the same processes that
have been discussed in talking about Tikopia. Neville would set up scope for
micro-experiences creating very strong forces cleaving pathological
entanglements, as well as forces forging functional bonds within and between
people. Typically, patients arrived with a very small family-friendship network.
Both the sociological category and the composition of
small groups varied daily. All the small groups at any one time were based on
the same category.
The social categories were:
(i)
age
(ii)
married/single
status
(iii)
locality
(iv)
kinship
(v)
social
order (manual, clerical, or semi-professional/professional) and
(vi)
age
and sex.
Friday’s
Small Groups were made up according to both age and sex for both staff and
patients. This was the one exception to the non-segregation policy. Often
inter-generational issues, including sexual abuse issues, were the focus of
these Friday groups.
People in pathological social networks would be all
together with everyone else in Big Group. However, because of the
continual changing composition in small groups, the members of these
pathological networks were regularly split up (cleavered) for the small group
sessions. Age grading was deemed very important, as it is one of the basic
divisions in society. Neville told me (July 1998) that the thinking was that
age grading sets a context for the production of personality changes to prepare
the client for life outside Fraser House. Age grading also allowed space for
sorting out inter-generation pathology that was very prevalent. For example,
Appendix 13 contains a note that at one time the Canteen was staffed only by
people under twenty years of age. This would have created scope for sustained
inter-generational relating with suppliers and customers.
Because of the number of categories, any visitor coming
regularly on certain days of the week would find that they would be attending
groups based on differing categories. For the small groups based on locality,
After a time at Fraser House these individual patient family/friendship
networks would expand to have members with cross-links to other patient’s
networks, and with a continual changing Unit population with overlap in stays,
these nested patient-networks became very extensive. As well, all these people
had Fraser House experience in common, and a common set of mutual support
skills. The critical role of locality and Neville’s use of locality in this
increase in the size and functionality of patient’s social networks is entirely
resonant with Indigenous links to place, and the significance of place and
placeform in Keyline.
CHILD-PARENT
PLAYGROUPS
Webb and Bruen (1968) wrote up research relating to the first 13
weeks of Multiple Child-Parent Therapy in Fraser House – called by some, ‘the
mad hour’. Median attendance was 15 parents and sixteen children (aged 14 and
under). This therapy was held in the same room as Big Group. All chairs were
removed and ‘free play’ items were provided - including saucepans, games,
balls, clothes as well as chalk and a blackboard. Attendance for parents and
their children under 14 was compulsory and doors were looked to prevent people
leaving; although parents with unproblematic relations with young infants were
not required to bring them. Outpatients visiting Fraser House with children
under 14 also attended the parent-child groups. As with other groups at Fraser
House, there was a spread of diagnostic categories[1]
among the people attending, as well as a spread of under-actives/over-actives
and the under-controlled/over-controlled (Bruen Dec, 2005).
The first half hour was a free period. Parents asked what
they were supposed to do. The only instruction was ‘parents are free to play
with or discipline their children as they see fit’. Staff were told that during
the free period they were to observe but not intervene unless physical damage
seemed imminent. Staff could move around and talk to parents or play with
children; however, staff were not to organize anything.
In the first few weeks these groups were extremely noisy,
rowdy and stressful for parents, staff and children alike, especially the free
period where staff were almost as overwhelmed as the parents.
The second half hour was usually structured with finger
painting or routine group therapy. The third half hour was a reporting session.
After that session the attendees were divided into three groups run by staff -
parents (one hour session), children 8-14 (one hour session) and younger
children (half hour session). The half hour with the younger children was
described as ‘utter chaos’. There was then a final reporting session for staff
for a half hour.
Initially, nearly all parents expressed considerable
hostility towards the group and towards the staff who set up the group. During
subsequent groups, parents grudging acknowledged that children enjoyed it. In
an email exchange Bruen stated (December 2005) that:
Even
having parents become hostile towards us succeeded in bringing them closer to
their children.
The free period was originally an arena for staff to
watch interactions that emerged. Initially parents were unable and unwilling to
go near or engage with their children – they were emotional strangers. ‘Getting
together’ as a family was a rare event in these people’s lives.
For six weeks the group was a provoking agent. After six
weeks parents grudgingly admitted that the children enjoyed the sessions (Webb
& Bruen, 1968, p. 52). After 9 weeks, successful whole family discussions
were starting. Parents began playing with each other and play was being
organised by parents with and between whole family groups. Whole families began
to get together and enjoy each other’s company. A major therapeutic role of the
groups was having parents showing pleasure and amazement in having for the first
time their children approaching them to play with them, and if parents did
this, that it would not have disastrous consequences.
During the thirteen weeks covered in the Web-Bruen
research, the attendees were also attending Big and Small Groups, and discussion
about the Child-Parent Groups was often raised in both of those forums.
Terry O’Neill used to facilitate this upstairs child-play
segment as a volunteer psychologist after Warrick Bruen left. (I received my
counselling skills training from Terry in the late Seventies.) Terry told me
(Oct 1998) that on his first evening alone with the children (8-14), so much
emotional energy had been generated during the first segment, ‘playing’ with
their parents, that the nature of the frenzied play upstairs was scary. Some of
the older children were kicking a soccer ball round like a deadly missile.
Everyone had to be super alert not to get his or her head knocked off. Terry
said (Oct 1998) that having a number of disturbed children in play therapy in
these evening sessions stretched his skills to their limit.
The substantial change towards good parent-child
relations during free play in these child-parent groups is another example of
‘provoking’ or ‘perturbing’ the families and tapping into functional self-organizing
aspects in the context of all of the other Fraser House changework.
INDIVIDUAL THERAPY
When deemed appropriate, face-to-face therapy between two
patients, a patient and a nurse, or a patient and a doctor was held. Even in
this individual therapy, the central focus was inter-patient relationships.
Encouragement was continually given to ‘bring it up in the group’.
While it was recognized that during some crisis times a
patient may need support by a doctor or nurse, most face-to-face therapy was
informally between patient and patient as they went about everyday life, with
the wider community always a background.
RESEARCH AS
THERAPY
Neville
commenced his postgraduate diploma in sociology shortly after Fraser House started
and completed it in 1963. Neville spoke (July 1998) of Fraser House being an
informal Post Graduate Research Institute, and of the Unit being the most
advanced Social Research Institute in Australia.
Neville had pointed out to me that Franz Alexander had
observed the potential for healing of the caring relationship between Freudian
analysts and patients (Alexander 1961). Similarly, Elton Mayo (Trahair 1984) had found in the Hawthorne experiments
amongst workers in the early part of this century, that the change component
was not so much the various ‘treatments’ of the research - rather that it was
that the researchers were acknowledging the workers’ dignity and worth and
showing an interest in them. Change was linked to the emotional experience of
being research subjects. Similarly to Mayo’s work, Fraser House patients and
staff were the focus of continual research by Fraser House researchers and the
outside research team headed up by Alfred Clark. Patients were being
continually asked to reflect on themselves, other patients, other staff, Big
Groups, Small Groups and on every aspect of Fraser House and aspects of wider society.
Through all of the research, patients learned about the difference between
quantitative and qualitative research as well as about the notions ‘validity’,
‘reliability testing’ and ‘trustworthiness’, and how these are very useful
notions as part of living in a modern community, especially one with extensive
pathology. Patients also became involved in both qualitative and quantitative
research data gathering as well as discussing the results and implications of
the research.
During 1963-1966, research by nurses in Fraser House was
supervised by Neville (Yeomans, N. 1965a, Vol. 12, p. 69). Neville gave preliminary training to nurses
in research methods and also trained the social worker in research methods. At
one time Neville arranged a Fraser House Research workshop with 25 associated
projects (Yeomans, N. 1965a, Vol. 12, p. 86-99). As an example, Fraser House residents were
involved in rating patient participation and improvement (refer Appendix 16).
In answering, patients were not only being encouraged to notice healing
micro-experiences (experience of little bits of behaviour that may contribute
to healing), they were receiving the strong positive emotional experience that
what they thought and felt about things mattered and was of value. Having come
from conflicted family environments where contradictory communication (Laing and Esterson 1964) was the norm, doing reality testing and
checking the practical usefulness, validity and relevance of their observations
was valuable. Patients and outpatients would start discussing a very diverse
range of topics and in the processes evolve their capacities in forming,
expressing and evaluating opinions and making insightful and useful
observations about human interaction.
VALUES RESEARCH
Another example of treating patients with respect,
dignity and worth was asking them to explore and give answers to questions
about their value systems. Neville carried out extensive values research (1965a) based on the concepts of Florence Kluckhohn (1953, p. 342-357). A list of the questions that were asked in
Neville’s Values Research is in Appendix 17. This Fraser House values research
was followed up by questionnaires being completed by over 2,000 people in
Sydney, Melbourne and Brisbane - the three largest cities in
In Neville’s view (Dec 1993), substantially shifting core
values amounts to shifting culture. Neville also stated that at the time, this
values research was, in all probability, the most extensive research on values
that had been done anywhere (Clark and Yeomans 1969, p. 20-26).
Appendix 18 and 19 lists inventories developed and used
at Fraser House (Yeomans, N. 1965a, Vol. 4, p. 43, Vol. 11). These inventories enabled the putting
together of a holistic psycho-social emotional mindbody portrait of each
patient and outpatient’s whole life, covering presenting matters, recent past,
post-school period, childhood, as well as work history and recreational
activity. This is consistent with the holistic socio-emotional focus of change
at Fraser House. Reflecting these stories back to patients engaged in
reconstituting their unfolding story had functional value.
Despite being extremely busy with every aspect of Fraser
House and its links into the community, Neville was very active in research and
writing up papers. He was an active presenter at conferences and other
professional meetings. Appendix 20 contains three Tables (A, B, and C) listing
fifty seven of the extensive body of Neville’s research papers and monographs
mentioned in his collected papers in the Mitchell Library. Many are undated
though come from the 1959-1965 period.
Group and crowd behaviour during big groups was a
constant research theme. For example, in a filenote called ‘Colindivism’ (1965a) Neville describes the interactive nature of
collective and individual behaviour in Fraser House.
Patients knew that all manner of data was being collected
about them relating to demographic and socio-economic data, length of stay,
participation by their friends and relatives and the like. Research outcomes
were discussed with patients.
Within
a connexity based Cultural Keyline frame it made absolute sense to connect
patients to the interconnection and inter-dependence of aspects of society at
large. Psychiatric patients and ex-prisoners were asked their attitudes towards
overseas trade with SE Asia, or about landscape planning and urban renewal in
Neville
told me (Dec 1993, July 1998) that a process he used to protect Fraser House
was that a number of research workers from
Bruen told me (Aug, 1999) that Margaret Cockett made
sociograms of networks within Fraser House using the concepts of ‘power’,
‘opinion leaders’, ‘leaders’ and ‘influence’. The conducting of this research
was later confirmed by Margaret Cockett (April 1999). Regrettably, this
research was among the materials discarded by
Sociogram based research in Fraser House recognised that
P.A.’s three primary landforms (main ridge, primary ridge and primary valley)
embody horizontal unity in the context of vertical cleavage though no reference
to Keyline is made. Neville and other researchers at Fraser House used the
above notions of horizontal unity in the face of vertical cleavage
in doing sociogram research into the friendship patterns among staff and
patients in Fraser house (Clark and Yeomans 1969, p. 131). A ‘glimpse’ of Neville’s use of Tikopia’s
cleavered unities is in Clark and Yeomans’ book, ‘Fraser House’ under the
subheading ‘Cleavages’ relating to the sociogram research (Clark and Yeomans 1969, p. 131). Not surprising, this sociogram based
research showed that Neville was only staff member:
with a link, by means of a mutual tie, into the
genotypical informal social structure…. (Clark and Yeomans 1969, p. 131).
Sociogram 1 Sociogram Showing the Friend Network in
Fraser House.
This
finding is fully in keeping with Neville’s notion of devolving responsibility
and reversing the status quo. It was also in keeping with Neville’s hands-off
though being profoundly and sensitively linked that he was enabler on the edge
of the informal social structure.
Apart
from research as therapy, Fraser House research served at least two other
functions. Firstly, the results were fed back in to modify the structure,
process and action research in the Unit. For example, the critical and
destructive role of extremely dysfunctional families and friends in holding
back patient improvement became clearer to staff and patients alike from both
experience and research over the first three years. Greater efforts were then
made to involve these networks. Secondly, the research was used to protect the
Unit and ensure its survival, at least for a time.
PSYCHIATRIC RESEARCH STUDY GROUP
Neville set up the Psychiatric Research Study
Group on the grounds of the
The Study Group provided a space where ideas
were enthusiastically received and discussed. Some participants had been
finding it hard to get an audience for their novel ideas within the climate of
the universities of the day. The Study Group was another cultural locality.
Anything raised in the Study Group that seemed to fit the milieu in Fraser
House was immediately tested by Neville in Fraser House. In trying something to
see if it worked, Neville spoke (July 1998) of ‘the survival of the fitting’.
At one time there were 180 members on the
Psychiatric Research Study Group mailing list. Neville wrote that the Study
Group:
…represents every field of the social and
behavioural sciences and is the most significant psycho-social research
institute in this State.
The Psychiatric Research Study Group
maintains a central file of research projects underway throughout NSW and acts
in an advisory and critical capacity to anyone planning a research project’ (Yeomans,
N. 1965a, vol. 4, p. 24).
Meetings were held monthly at first at Fraser
House and then elsewhere.
WORK AS THERAPY
The canteen provided one context for using
work as therapy. Another example was the patients winning a contract to build a
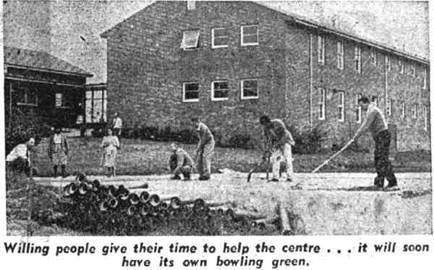
Photo
1 Patients building the Fraser
House bowling green in the Sixties - a photo from the Sydney Morning Herald (11
April 1962).
The
above photo accompanied an article entitled ‘The Suicide Clinic’.

Photo
2 I took this photo in June 1999 showing brick retaining wall and
Bowling Green behind the wire-mesh fence
The
above photo shows the Bowling Green area behind the fence that was levelled out
by patients with hand tools. The retaining wall was also built by the patients
and it has stood the test of time - still vertical. To reaffirm, a very important type of work
that some of the patients became very adept at was being therapists and
co-therapists in group and everyday contexts. All my Fraser House interviewees
confirmed (Aug, 1998 and April, 1999) that often the most insightful therapy in
everyday life and groups within the community was by patients.
Patient
based therapy was offered though the letter from the President of the
Parliamentary Committee (the letter is included as Appendix 11) (Yeomans,
N. 1965a, Vol. 2, p. 11).
MARGARET
MEAD VISITS FRASER HOUSE
The Anthropologist Margaret Mead visited
Fraser House as the Co-Founder (1948) and ex-President (1956/7) of the World
Federation for Mental Health (Brody 2002).
Separate discussions with Margaret Cockett and Neville (Aug, 1999)
cross-confirmed the following material about Mead’s visit. Margaret Cockett
informed me that Margaret Mead was introduced to Fraser House by an
anthropologist friend of Margaret Cockett in the NSW Housing Department who had
told Mead about Fraser House when Mead came to visit her. Cockett told me that
initially Margaret Mead could not believe what she was hearing and came to
Fraser House to check it out for herself. Mead was escorted throughout the day
by Margaret Cockett, the Fraser House anthropologist psychologist. Margaret
Cockett recalled Margaret Mead saying that she was very taken with the concept
of therapeutic community and had visited many such communities in different
places.
Mead very ably conducted the morning Big
Group and ran a small group when she visited Fraser House (discussion with
Neville, April 1999 and Margaret Cockett April 1999). Margaret Cockett
described Mead as being ‘absolutely on the ball’ in the role of leader of both
Big Group and one of the Small Groups. Margaret Mead also took the regular half
hour staff group meeting that followed the Big Group.
A
number of senior people from the health department joined Margaret Mead for
lunch where according to Margaret Cockett, Margaret Mead held court and
demonstrated that she was clearly ahead of every one of them in their
respective specialist areas. Margaret Cockett suspects that it was Margaret
Mead’s glowing report to these people in the NSW health establishment hierarchy
that made things just a little easier for Fraser House for a while. Neville
said (April 1999) that at that time Mead visited Fraser House, the medical and
psychiatric profession saw no relevance whatsoever for anthropology in their
professions. Margaret Mead gave the ‘big thumbs up’ to Fraser House to these
Department Heads, ‘heaping praise’ on every aspect of the Fraser House
therapeutic community.
Margaret Mead also chaired the Psychiatric
Research Study Group when she visited Fraser House (Yeomans, N. 1965a, Vol. 12,
p. 68).
Dr.
Margaret Mead, world famous anthropologist who visited Australia last year
attended a meeting of the Psychiatric Research Study Group and also stated that
she considered Fraser House the most advanced unit she had visited anywhere in
the world (Yeomans, N. 1965a, Vol. 12,
p. 69).
All
of my informants spoke of the dense holistic inter-related ‘total’ nature of
Fraser House. Neville (Aug 1999) told me that Mead also stated that Fraser
House was the only therapeutic community she had visited that was totally a
therapeutic community in every sense. Cockett, in talking about Mead’s
feel for Fraser House’s totality and completeness said that Mead spoke of
Fraser House as the most total therapeutic community she had ever been to.
(Note that the above sense of ‘total’ differs from Goffman’s use of ‘total’ as
a term describing entities like monasteries, prisons, asylums, and warships
that bracket people off from everyday life. While a ‘total institution’ in
Goffman’s terms (1961), Neville said that Mead was particularly taken with the
fact that important others were required to regularly visit patients in Fraser
House, and that one patient, having a horse as the only ‘important other’ in
her life, was allowed to have the horse tethered grazing on the lawns of the
hospital just outside Fraser House. A few other patients had a cat or a dog as
their ‘important other’. I took the photo below in August 2000. It shows Fraser
House through the trees and the grounds outside Fraser House where the horse
grazed.

Photo 3 A photo I took in June 1999
of the place where the horse grazed at Fraser House
Reading the Fraser House Committee Structure
(Appendix 13) may give a further feel for the totality and completeness that
Margaret Mead, spoke of when describing Fraser House as the most Total therapeutic
community she had ever been to.
Margaret Cockett (Aug, 1999) and Neville (Dec
1993 and August 1999) confirmed that Mead also stated that Fraser House was the
only therapeutic community that was totally a therapeutic
community in every sense. Similarly, in the forward of Clark and
Yeomans’ book about
Fraser House, Maxwell Jones, the pioneer of therapeutic communities in the
Throughout the book is the constant awareness
that, given such a carefully worked-out structure, evolution is an inevitable
consequence
(Clark and Yeomans 1969, Forward, p. vi).
It is this ‘total’ aspect of Fraser House
(and
Recall that Maxwell Jones had said of
therapeutic community in the
It does not amount to a treatment methodology
in its own right but complements other recognized psychotherapeutic and
pharmacological treatment procedures (Jones 1969, p. 86).
Neville had created a total therapeutic
community where every aspect was transformative.
To continue the theme of setting up
inevitable change in self-organising systems, I will now detail my findings
about Cultural Keyline.
Margaret
Cockett (Sept 2004) told me that Neville and everyone connected at Fraser House
where constantly trying out new things. Everything was extremely fluid. Someone
would come up with an idea and it would be immediately woven in. In Margaret’s
view Neville tended to make connections between some
new thing they were trying out and what they did on the farm. It seems that Neville’s sensing of what
Keyline adapted to the psychosocial may be, emerged out of Fraser House’s
dynamic eclectic process rather than being an intellectual exercise imposed on
Fraser House. Theory emerged from theorein (pretheoretical theorising) (Pelz 1974) and process.
Neville
first mentioned the term ‘Cultural Keyline to me when I was staying with him in
Yungaburra in December 1991 and when I asked Neville to expand on what he meant
by the term, Neville changed the topic saying that I already knew all about it.
I was puzzled by this. I again asked in December 1993 and he told me to read
all of his father’s Keyline writings and then I may discover Cultural Keyline
in my own actions. After his death in May 2000 I realised that Neville was
aware that through his subtle modelling of his behaviour in my presence, I had
absorbed aspects of his way and regularly used Cultural Keyline in my action
research in his presence, even though I did not know my actions were consistent
with Cultural Keyline. I sense that Neville’s view was that head knowing alone
will limit understanding of Cultural Keyline – understanding has to emerge
through the embodiment of values-based relevant experience.
My sense of ‘Cultural Keyline’ is that it is
of a matching form to the enabling interaction the Yeomans family had with all
of the myriad interlinking aspects of the soil, air, water, nutrient, and
warmth on their farms. Every aspect of the design and redesign of the Yeomans’
action on their farms was pervasively integrated. It was, to use Neville’s
phrase again, the ‘survival of the fitting’. Neville and his father knew that
it was virtually impossible to control a living system. Neville and his father
keenly attended to how the natural systems ‘worked’ on the farm and designed
their interventions to maximally fit with nature and allow nature’s emergent
properties to do what they do so well. P.A. and sons Neville and Allan (and
later, Neville’s younger brother Ken) would give the soil subtle enabling interventions
and perturbations, and then they would let the system self-organize towards
thriving.
Living systems have self-organization as an inherent property (for example, the
‘informal organization’ and the ‘grapevine’ in bureaucracies).
Neville
knew (June 1998) that living systems can reach a point, called in complexity
theory (Capra
1997, p. 167),
a bifurcation point, where there can be a sudden system negentropy (the
opposite of entropy) leading to the potential and emergence of sudden whole
system transcending transition to higher and more unpredictable complexity and
improved performance. The Yeomans had first-hand experience of how perturbation
and bifurcation work in nature in producing sudden whole system shift to a new
order of higher complexity (Capra
1997, p.28). The massive increase in detritivores in
their soil was one example. In the Fraser House context two examples of a
birfurcation point was firstly, when Neville went berserk in Big Group such
that the Unit survived well in his absence (Appendix 14), and secondly was when
Neville geared up the Frazer House community to support the 12 year old girl
(Appendix 15). In both cases Neville created a rich context where the Fraser
House social system jumped to a far richer mode of interacting. In each of
these cases Neville’s action was consistent with Pascale, Millemann and Gioja’s
(2000)
behavioural pattern in their book ‘Surfing the Edge of Chaos’:
Amplify
survival threats and foster disequilibrium to evoke fresh ideas and innovative
responses (2000, p. 28.)
Creating
contexts rich with potential for self-organising negentropy is very different
to laissez faire management where there is a hands-off approach.
Neville
applied these Keyline understandings in evolving Fraser House. In mirroring
Indigenous way, Fraser House was about fostering respectful co-existence and
meaningfully surviving well together. Everything Neville did in Fraser House
was designed to fit with everything else - naturally. Everything complemented and
supported other aspects. Things that did not work were fine-tuned or discarded.
Issues that arose in one context were resolved, or passed on to other contexts.
In Fraser House, what worked (as well as problematic aspects) was discussed
with everyone in Big Group. Issues not resolved in Big Group were passed on to
Small Groups and vice versa. Issues within Committees were resolved, or passed
on to Parliamentary Committee. Issues within the Parliamentary Committee were
reviewed by the Pilot Committee. This pervasive inter-connected weaving of
everything with everything is why Margaret Mead said it was the most
complete therapeutic community she had ever seen, and why Maxwell Jones
said that participants in Fraser House had to change.
Subsequent
to Neville’s death in May 2000, l identified four non-linear interconnected
inter-related aspects of Cultural Keyline:
1. Attending and sensing self organising,
emergence, and Keypoints conducive to coherence within social contexts
2. Forming cultural locality (people connecting
together connecting to place)
3. Strategic design and context-guided
perturbing of the social topography
4. Sensing and attending to the natural social
system self-organising in response to the perturbing and monitoring outcomes
Keyline is a model of sustainable
agriculture. Cultural Keyline is model for sustaining wellbeing based human
inter-acting and inter-relating. As Keyline fosters emergent farm potential,
Cultural Keyline is a rich way of fostering emergent and thriving potential in
social systems. A short summary of my findings relating to Neville’s Cultural
Keyline process in action follows. The following process is non-linear with
connexity between all of the following aspects. Some repetition reflects
fractal aspects, for example between sensing and designing.
Attending and Sensing
·
Attending
very closely to the features of the ‘social landscape’ in unfolding social
contexts
·
Being
open, surrendering and receiving all aspects of the social topography - sensing
the information, meanings and the issues in the forms, and not laying on it any
of our own projections
·
Sensing
each person, family, network and community as a self-organizing living system
·
Sensing
the connexity (interconnected interdependence) in the psycho-social topography
·
Sensing
the free energy and context role-specific functional behaviours in everyone
involved
·
Sensing
the information distributed throughout the system and recognising how this
information is concentrated and merges at the Keypoint – information about
mood, theme, value, interaction and unfolding outcomes - sensing their
inter-connectedness within the whole of what is happening.
·
Sensing
the fractal Cultural Keypoint(s) in the unfolding context - where these
energies and information (mood, theme, value and interaction) meet and
concentrate (just like the fractal quality of discrete information distributed
in each of the three land forms all meeting at the Keypoint), and have emergent
potential for social cohesion – and sensing the connecting theme(s) that
merge(s) from the concentrate – the theme(s) that has/have potent significance
for all in the unfolding context (whether participants realise it or not).
Forming Cultural Locality
·
Interacting
with the surrounding locality as a living system
·
Offering
to support people as a resource
·
Enabling
cultural locality – first the gathering, then the nexus towards community and
placemaking
·
Enabling
and fostering self-help and mutual-help
·
Enabling
others to tap into personal and interpersonal psychosocial and other resources
Strategic Design and Context-guided Perturbing of the Social
Topography
·
Unfolding contexts telling us what to do next
·
Enabling contexts where resonant people self organize in mutual
help
·
Fostering and enabling resonant grassroots networking in the
region
·
In
the unfolding context, sensing the inter-connectedness of mood, theme, value
and interaction; sensing the Keypoint where these meet and concentrate – and
sensing the connecting theme that merges from the distributed information
·
Engaging
in context appropriate perturbing at the Keypoint – from gentle to full on
perturbing - to evoke Keylines of interaction on the theme and associated mood,
values and interactions
·
Taking
the time and ensuring the sustaining of the Keypoint theme along the Keyline
till the turning point (potentially towards a new Keypoint theme), and then
recognizing and shifting to that Keypoint theme. If no Keypoint theme emerges,
then working with the free energy, or
·
Using
the Keylines of interaction as a guide to further engaging in action
Leaving Nature to do the Work
·
Sensing
and attending to the natural social system self-organising in response to the
perturbing
·
Honouring,
respecting, holding and leaving free the space and place for individual,
family-friendship networks and community re-constituting to happen
·
Having
faith in the thriving of living systems and knowing when to leave it to
self-organize and naturally do what it knows best - towards constituting/re-constituting
wellness
A
case study of Neville using Cultural Keyline is Appendix 14 (Going Berserk).
Neville
and his father were never into laissez faire management – having a non-involved
hands-off approach. When Neville travelled overseas he left in place a system
operating on the above four Cultural Keyline aspects. A group of people had
taken on his enabling role that entailed context specific tight control and
freedom and pervasive attending and sensing.
Neville
turned himself into a Keypoint. Metaphorically Neville placed himself in
society at the junction of three forms of social topography – the psychiatric
bureaucracy, the media, and the marginal fringe from the backwards of asylums
and no-parole prisoners. Within three years, Fraser House marginal residents
were training trainee psychiatrists in the new area of community psychiatry.
Neville became a zoologist, doctor, psychiatrist, sociologist, psychologist,
and barrister. Placing all this academic reflection within himself he placed
himself as head of the psychiatric study group associated with Fraser House. He
positioned the Study Group linked to Fraser House as the premier social
research facility in
My
understanding of the links between the farms and Fraser House are set out below:
No
one I interviewed for this research knew anything about Cultural Keyline;
Neville had never mentioned the term to them. While Neville never specifically
mentioned Cultural Keyline in any of his writings, the concept is implicit in
many of them; as an example, refer Appendix 4 – Neville’s forward to his
father’s book ‘
Cultural
Keyline themes implicit in Neville’s Forward:
·
Change
in values
·
Bio-social
survival depends upon harmonious working with nature
·
·
Landscape
must be husbanded with loving care
·
The
beauty and freedom of personal space depends upon caring for the integrity of
all our environment
Yeomans Farms Fraser
House
|
||
|
|
|
CULTURAL KEYLINE IN GROUPS
In
socio-morphological terms, a key role of the group facilitator was to
constantly scan for the ‘lay of the land’ in the group. This section extends
the above material on the use of themes as Keylines of discussion in Big Group.
A group of Fraser House patients wrote about how interest in themes was used in
groups – one version of this text included as Appendices 7 and 8 (Yeomans,
N. 1965a, Vol. 4, p. 17-20).
Big Group and Small Group themes emerged from the unfolding social topography in
the group. Themes were not concocted by group leaders and imposed. Themes are
where key issues for all in the group coalesce. Themes, as social coherence
amidst chaos, would arise from the context and often be self starting, or only
needing the slightest nudge to get underway. Once started on a coherence theme,
all participants tended to be hooked into their links to the theme.
Neville would place a metaphorical dam just below the Keypoint that would hold
the energy on the theme, and let the interaction move, as appropriate to
context, along the Keylines of discussion (metaphorically just downhill of the
contour as in Keyline ploughing) so that it moves with assistance of group
momentum (gravity).
Once
a theme was energised in Fraser House groups, and the theme was considered to
be not too superficial or inappropriate, the group may pay some attention to
it, and the suggested or emergent theme may be selected as ‘the Big Group
theme’ for an ensuing period during that hour. This theme would then not be changed
to another without good reason (Appendix 8). Interest in a theme may be viewed
as an attractor that determined the ‘flow’ of attention from ‘all directions’
near the ‘ridges of high potential energy’ to the ‘Keypoint’. Within Fraser
House Big and Small Groups, both interest and theme were emergent phenomena.
Interest (from the Latin: ‘to enter into the essence or God energy’) in
the theme becomes the Keypoint (literally and sociomorphically) for a time in
the Big Group social topography. The theme becomes the Keyline of discussion
for a time, and thematic psychosocial emotional energy in flow may be
transferred through the Big Group topography via ‘individual channels parallel
to the Keyline’ through the people topography. The word ‘theme’ is from the
Greek ‘thema’ meaning ‘motif; recurrent idea; topic of discussion or
re-presentation’.
The
following notes on interest in the theme is from the Fraser House Staff
Handbook (Appendix 7):
If
most of the group is involved in interaction, it goes without saying that they
are also interested. However, interest can be very high even though there is
not much interaction. Look at their faces, their feet, their hands, their
respiration, the way they sit, and it will be known if they are interested or
not (Yeomans,
N. 1965a, Vol. 4, p. 17-20).
The
Staff Handbook (Appendix 7) also notes the interaction between the
facilitator’s process and the theme, mood, interest, tension and the unfolding
interaction.
Resonance
between all attendees and the theme flowed from the theme having the inherent
property of being conducive to social coherence. To put this into context –
this was with a group of people who were the very mad and the very bad. The
group was filled with polarity – the under active and the over active, the
under controlled and the over controlled, as well as the under anxious and the
over anxious. There were colluding factions and unreachable isolates. In this
dysfunctional tangle there continually emerged themes that held everyone’s
interest – that everyone resonated with – that is, themes ‘conducive to
coherence’. Attendee resonance was supported by the theme-based connexity in
the cultural locality topography.
Group facilitators would specifically watch
for attempts to change the theme. In the patient’s write-up about the use of
interest in themes in Fraser House they wrote that attempts at changing the
theme:
……may be done deliberately by a patient for a
fairly obvious reason (such as a personality clash with someone involved in the
current theme), or a less obvious reason such as an unconscious identification
and a consequent wish to avoid the theme. It may also be done through plain
insensitivity on the part of the person making the attempt at the change. There
are many reasons for these moves, and it is the therapist’s role to decide on
the dynamics of the situations and then to make use of them by feeding them
straight back into the group at the time, and if necessary, to make an
interpretation of the dynamics operating in the events and occurrences’
(Appendix 7).
As more than one Keyline theme may be either
jostling for attention or potently latent in the ebb and flow of Big Group
energy, Neville’s skill was to identify the most potent one in the unfolding
context – perhaps the one that subsumes a number of the other presenting
Keypoint themes that then may become sub-themes as Keylines of engagement.
Neville passed on this skill to other Big Group facilitators and to me and
others who worked with him in action research.
Recall that there is only one Keypoint per
primary valley. Diagram 2 shows that Keypoint
in different primary valleys are often on different contours with different
potential energies in the respective valley systems. The Keyline only goes
along the contour through the Keypoint till the change of curve (refer diagram 2 in Chapter Five). Isomorphic with
Keyline, the next Cultural Keypoint theme may be at the same, or a higher or
lower contour and associated level of potential energy - so the group
facilitator would note this information in the social milieu in shifting themes
and work with the new energy. There were all manner of competences and nuances
associated with the shift of thematic keypoint in Fraser House groups and how
to work with the change in energy.
Peopling the
Topography – Sensing Cultural Keyline at the Keypoint
In 2006, I spoke with Terry Widders about
visiting Watsons Bay to sense Cultural Keyline at a Keypoint. Terry spoke of
‘peopling the topography’ and exploring the ‘contours of peoples’ minds’.
Taking up Terry’s suggestion I went to Watson’s Bay (refer Photo 24) with my
son Jamie.

Photo 4 Watson’s Bay Topography - compile made by me
from photos taken by tourist and sent to me October 2005 – used with permission
Recall Neville’s strategic use of locality
mentioned in Chapter Seven. Photo 2 reveals Watsons Bay’s topography. The
Watsons Bay Festival was in the park (The green area in the centre right of the
photo). The park is located in a primary valley below the main ridge and
between two primary ridges. The festival focal point was at a Keypoint in the
primary valley. The festival’s Keypoint theme was ‘celebrating life”. Neville
intentionally placed this celebration of life sixty metres below where
Sydneysiders go to suicide at The Gap. The bus in the photo is parked where the
Fraser House little red bus used to park two years earlier when the Fraser
House patients made crisis calls to stop suiciders.
Jamie and I came to Watsons Bay Park by ferry
and walked up to the Keypoint which is to the right of the path walking up.
Following Terry Widders suggestion, we decided to people the topography by
role-playing potent scenarios from our lives together. We did this while
standing at the Keypoint. In this we were modelling the position Neville took
when he was for instance leading Fraser House Big Group. Jamie and I separately
found where the different players in these re-enactments were located in the
Watsons Bay topography. When we compared where we sensed people were, we found
that we had complete agreement. For both us, our clarity about people’s
placement was inexplicable. Where we sensed them was definitely where they
were; people were definitely not in any other place in the surrounding
topography. Some were in the middle of the bottom of the valley. A few were
above us on the main ridge. Some were on one or other of the primary ridges.
Most were some distance from the Keypoint.
We sensed the themes that were conducive to
coherence in these people. We sensed the located people’s differing energy,
emotion and interest, and how these were linked to the Keypoint theme in the
scenarios. We sensed the nature of the interaction, mood and value mix that may
sustain interest and cohesion.
We also sensed the compaction in the social
topography, and how this compaction was sustaining fixed patterns of
dysfunction. We sensed the possible role-outs from perturbing the compaction,
from chisel ploughing the social terrain. We sensed the effect of this on
‘water’ flow as energy exchange. We sensed how this may flow gently through the
social system without eroding rush from the main ridge, and gently flow out
towards the primary ridges and be received throughout the system. We sensed the
effect of this dynamic on the unfolding of theme-based interaction. We noticed
how some people changed their positions as the scenarios unfolded, and the
effects of this change on the person and his/her interactions with self and
others. We then moved to the high point on the ridge (where photo 24 was taken)
to get another perspective. Neville would also do this to get the big picture.
We returned to the Keypoint and walked and sensed the Keyline. Then we
descended along one of the primary ridges to the bottom of the valley, sensing
the scenarios from the different locations, and as we placed ourselves on
others’ places.
I understand the above process has resonance
with Indigenous way. The richness of this embodied sensing of located
interactions only comes from doing it at a Keypoint and in and around the
topography.
SUMMARY
This
chapter has explored the many change processes evolved at Fraser House.
Neville’s adapting of Keyline to Cultural Keyline has been detailed. The next
chapter introduces criticisms of Fraser House and Neville, and includes a
response to these. The processes Neville used to spread Fraser House way into
the wider community and to phase out Fraser House are described. The chapter
concludes with a brief discussion of ethical issues in replicating Fraser
House.